Expansion 4.0: Graftless LMSF with screw expanders — case 1.6/1.5
TL;DR — Clinical case at sites 1.6 and 1.5: residual roots, low maxillary sinus floor. Two implants placed simultaneously with the LMSF (Localised Management of Sinus Floor) technique, calibrated screw expanders, graftless approach. Definitive prosthesis after healing. No biomaterial, no lateral window.
Premise
My father called it Localised Management of Sinus Floor. LMSF. It was 1998, International Journal of Oral & Maxillofacial Implants,¹ with Scipioni, Calesini, and myself. A case series of 499 implants in 303 patients, 97.5% survival rate by Albrektsson criteria (which were the standard at the time).
The idea was simple. And with the implants available at the time, it was also the most logical. If the ridge is thin and the sinus is low, you do not need a lateral window. You can expand the buccal cortical plate, elastically lift the bony floor of the maxillary sinus, and place the implant: all from the alveolar crest, through the same access. One flap, one direction, one session.
Twenty-eight years on, the technique is still there. But the instruments have changed, the way of thinking about the technique has changed, the availability of CBCT has changed. The principle has not.
This article tells a recent case — sites 1.6 and 1.5 — performed with what I call, between us, Expansion 4.0: the contemporary version of the family technique.
What changed from 1.0 to 4.0
Four generations, one logic.
1.0 — Edentulous Ridge Expansion (Scipioni, Bruschi, Calesini, 1994).² The frontier was to expand the thin ridge, without grafting, and place the implant simultaneously. Instruments: chisels and hand-percussion osteotomes.
2.0 — Localised Management of Sinus Floor (Bruschi, Scipioni, Calesini, Bruschi, 1998).¹ The same logic, extended to the sinus. The “greenstick” fracture of the sinus floor becomes the key to gaining height without opening the maxilla.
3.0 — Replacement of hand-driven osteotomes with magnetodynamic percussion osteotomes.
4.0 — It is the synthesis I practise today. Screw expanders, graftless approach, management of the immediate post-extraction case in a single session. Whatever does not need to be added, is not added. Whatever biology can do on its own, we let it do.
The leap from 3.0 to 4.0 is conceptual before it is technical: stop believing that the lift needs a traumatic system to work. In reality the technique is linear, simple, free of nuisance for the patient.
Lundgren³ had already written it in 2004 — the elevated sinus membrane creates a secluded compartment for bone formation.
For the general framework of expansion, the parent article is here: Ridge Expansion: The Bruschi-Scipioni Technique.
The case
Patient. Healthy woman, ASA1, sixth decade. Negative history for systemic disease and sinus pathology. Hygiene reinforced after initial preparation and motivation. Expectation: a fixed solution that lasts.
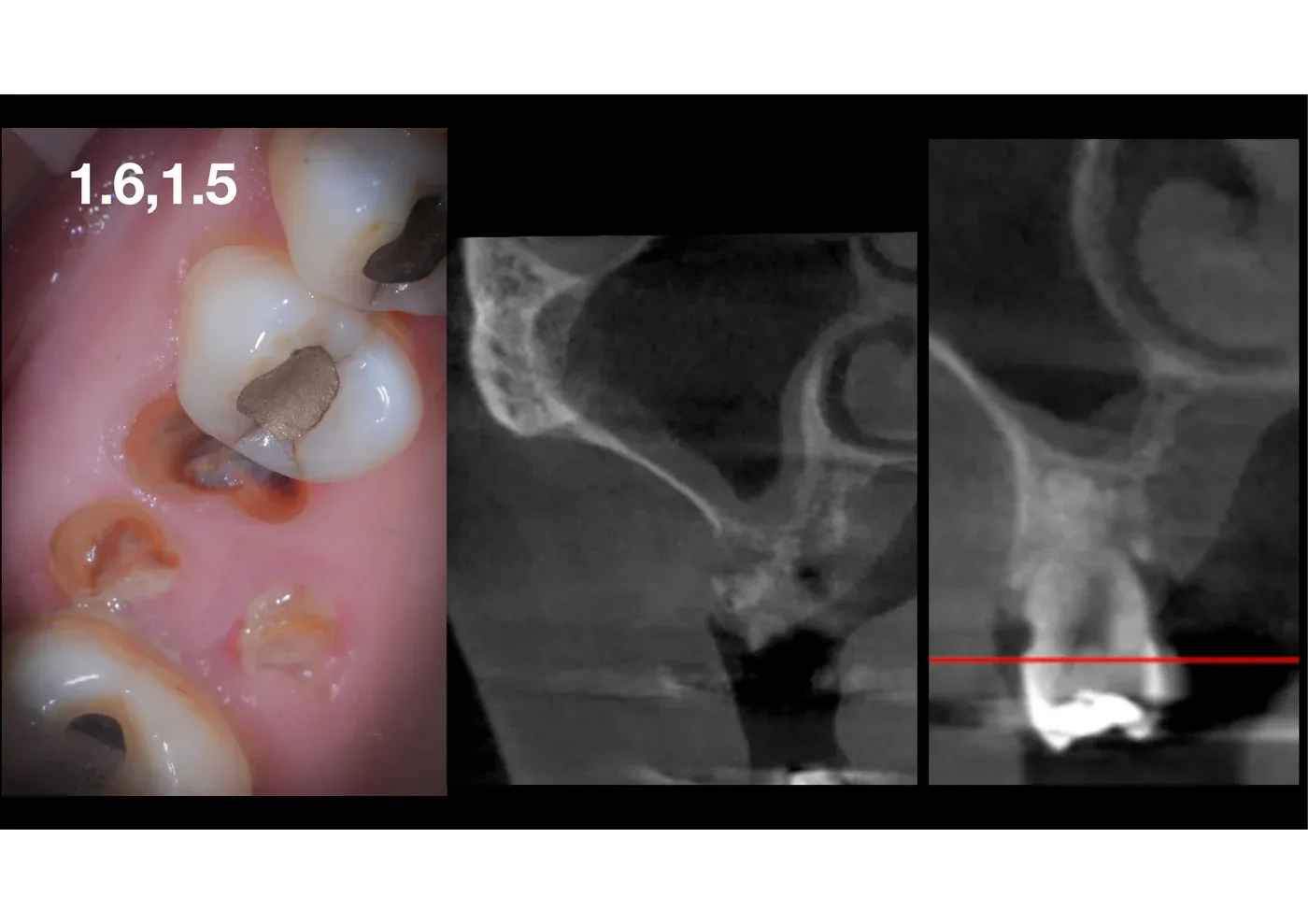
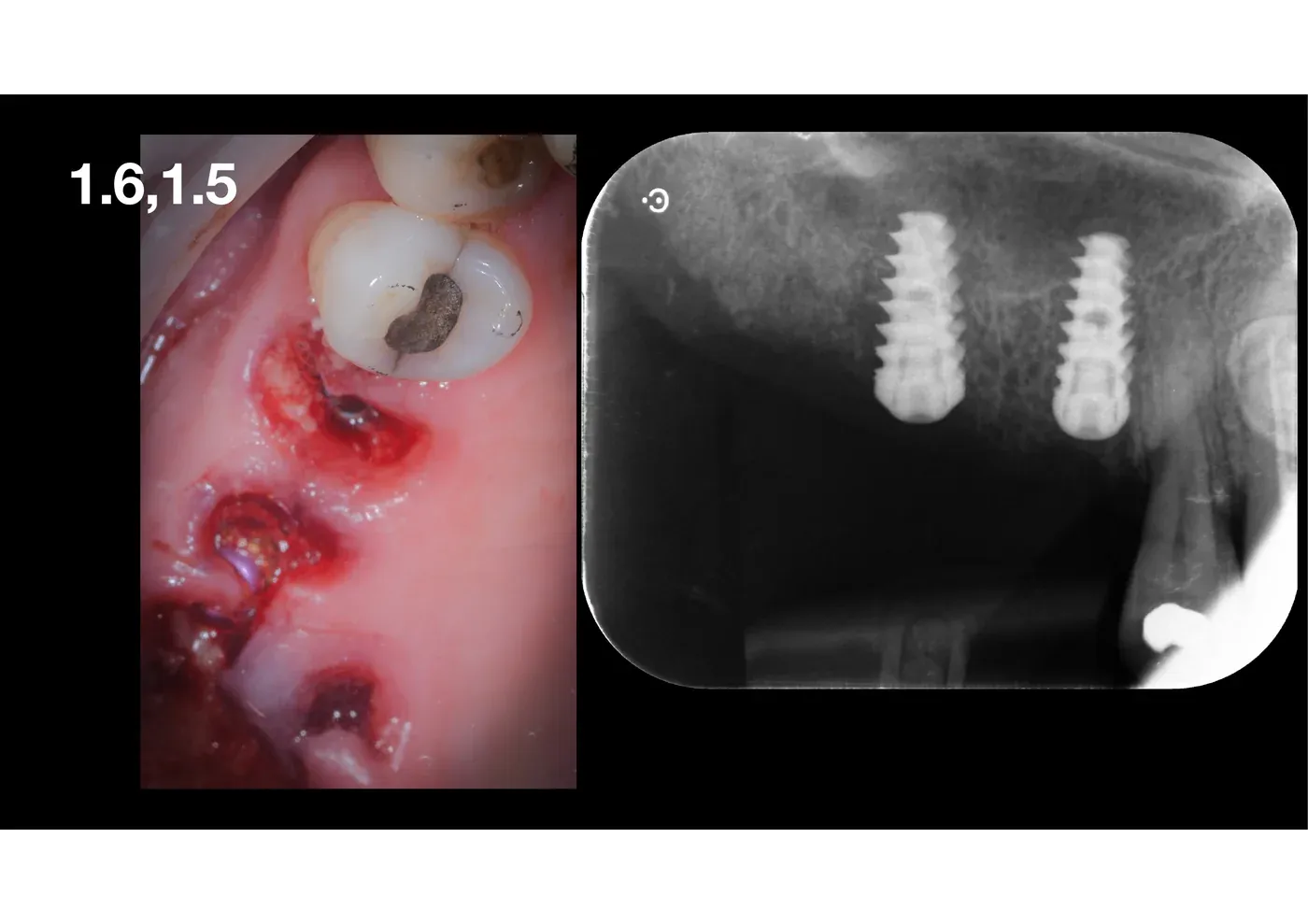
Local diagnosis. 1.6 and 1.5 with severe coronal destruction, non-restorable residual roots. CBCT: low sinus floor, residual bone height under the roots around 4-5 mm, intact membrane, no signs of sinus inflammation. At the first molar, the low sinus floor is accompanied by extensive 360° demineralisation around the residual roots.
Plan. Atraumatic extraction of the residual roots. Graftless LMSF simultaneous to the two sites. Two implants placed in the same surgical session. Deferred loading.
Surgical steps
Partial-thickness flap. Preservation of the periosteum on the buccal cortical plate. Not negotiable: it is Stricker’s rule, it is the family rule. The periosteum is the vascularisation of the bone we are about to displace; if you lose it, you lose the expansion.
Extraction. Thin elevators, no leverage on the bony fulcrum. The buccal cortical plate must remain intact: it has to stay alive.
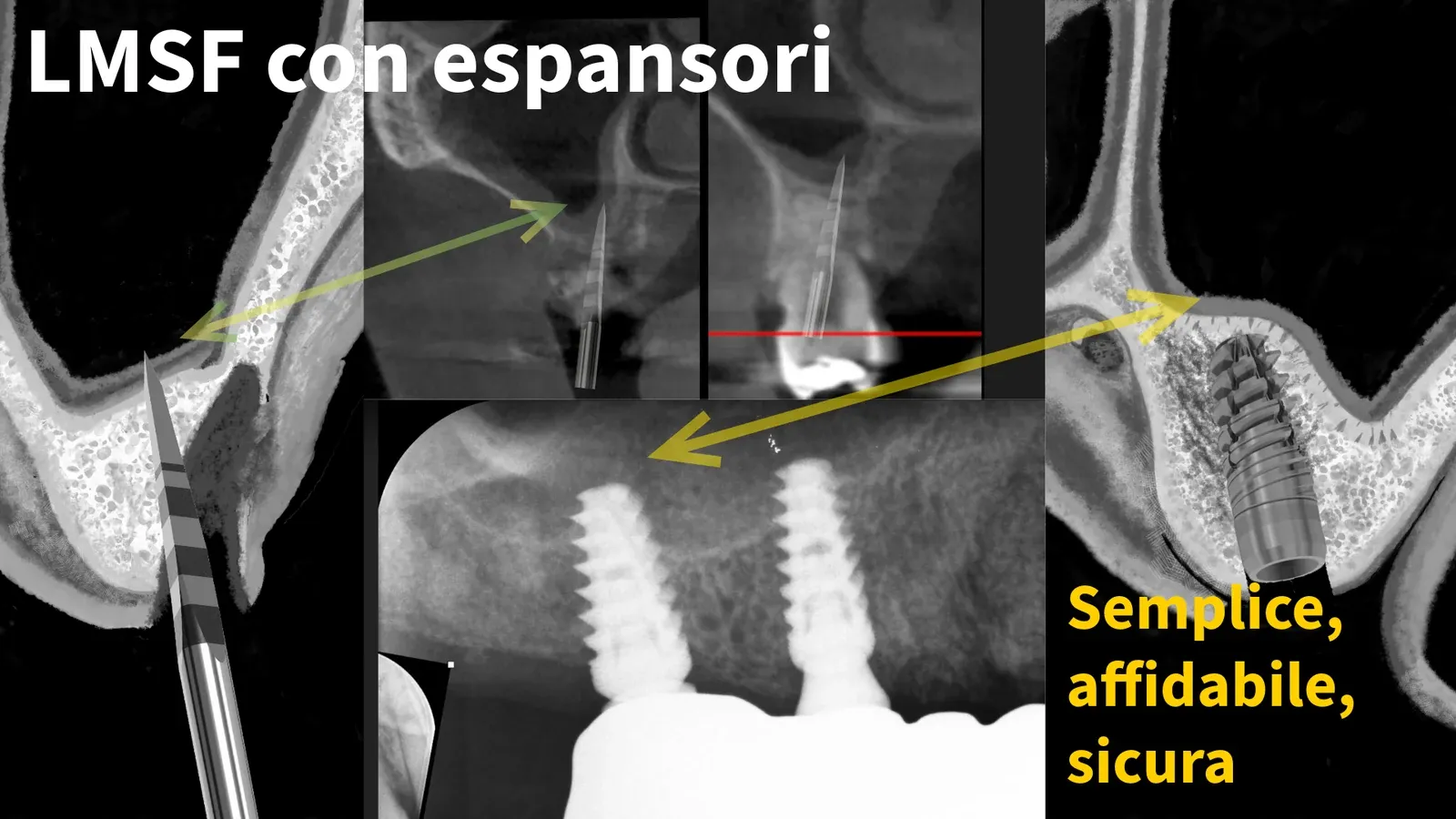
Crestal expansion. Calibrated screw expanders of increasing diameter. You screw slowly, you wait, you let the cortex yield elastically. Every half-turn is a listening.
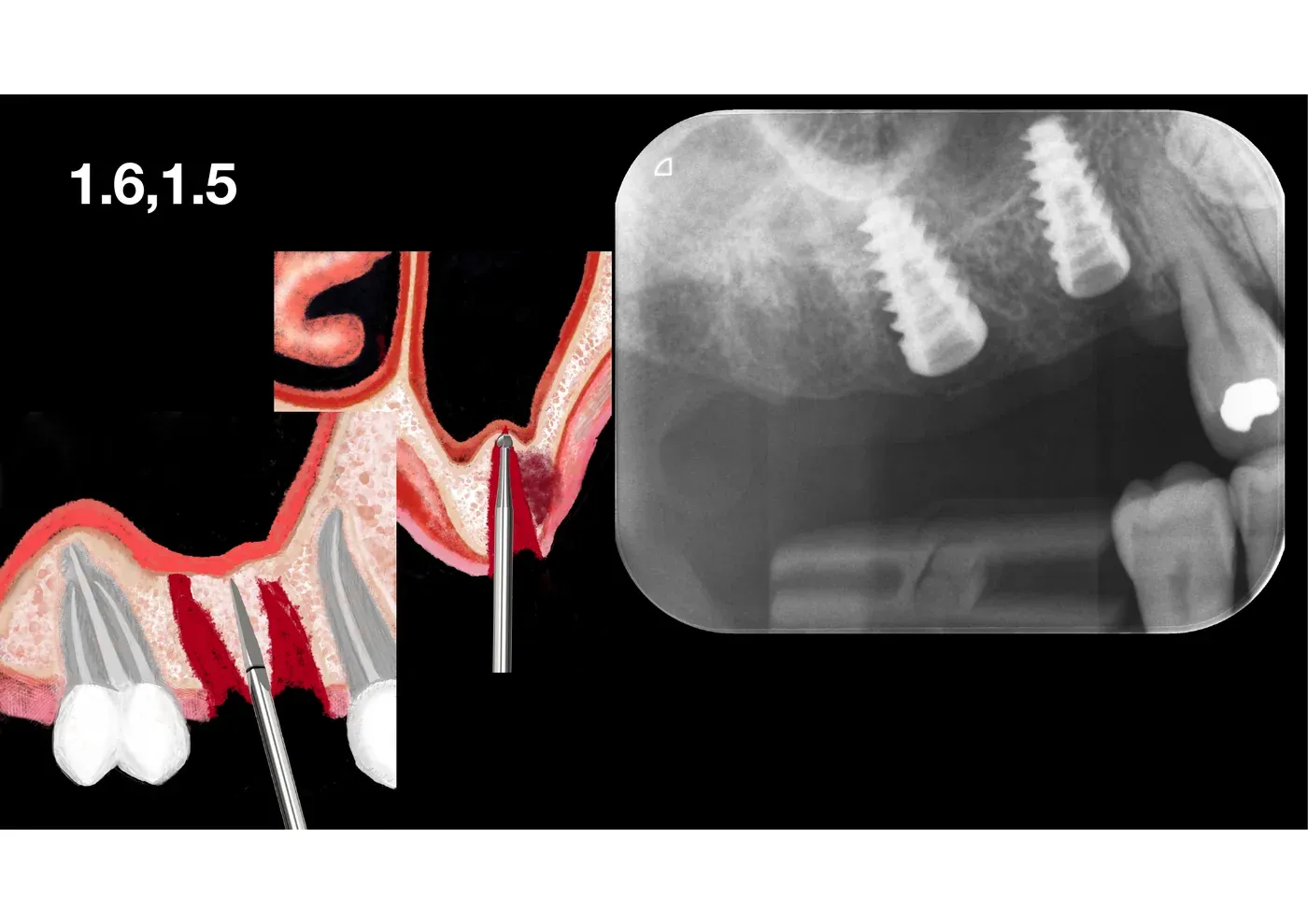
Localised management of the sinus floor. The expander reaches the sinus floor and goes past it (always lifting the bone as well, not just the membrane) by a few millimetres, checking the integrity of the sinus floor with the Valsalva manoeuvre. Bone rises together with the membrane above, pushed up by the clot and by the conical geometry of the expander. No instrument dedicated to the lift: the same expander that widened the ridge lifts the sinus floor.
Implant placement. Two implants of classic osseointegrating design, length chosen according to the new bone bed (apex at least 2 mm beyond the original position of the bony floor to stabilise the lift). Primary stability above 50 Ncm.
Closure. No suture. No graft, no membrane. Nothing.
Healing
Four months of waiting. Favourable course — no marked oedema, no pain worth prolonged painkillers, no positional vertigo. It is one of the advantages of 4.0 over 3.0: screwing replaces the mallet, and with the mallet goes the risk of post-surgical vertigo. Benign paroxysmal positional vertigo (BPPV) is the most common cause of vertigo, and it is due to the detachment of calcium crystals (otoliths) in the inner ear.
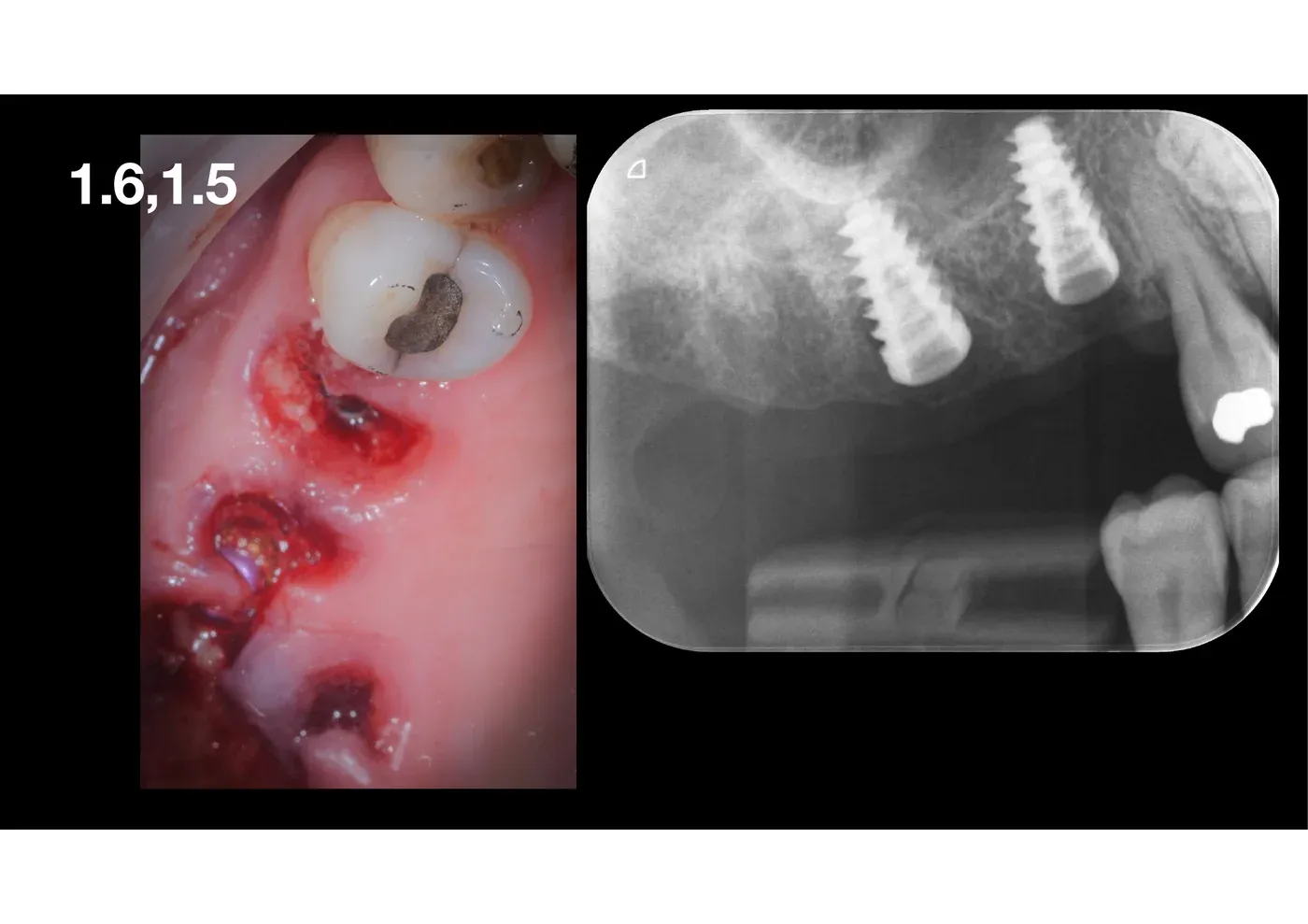
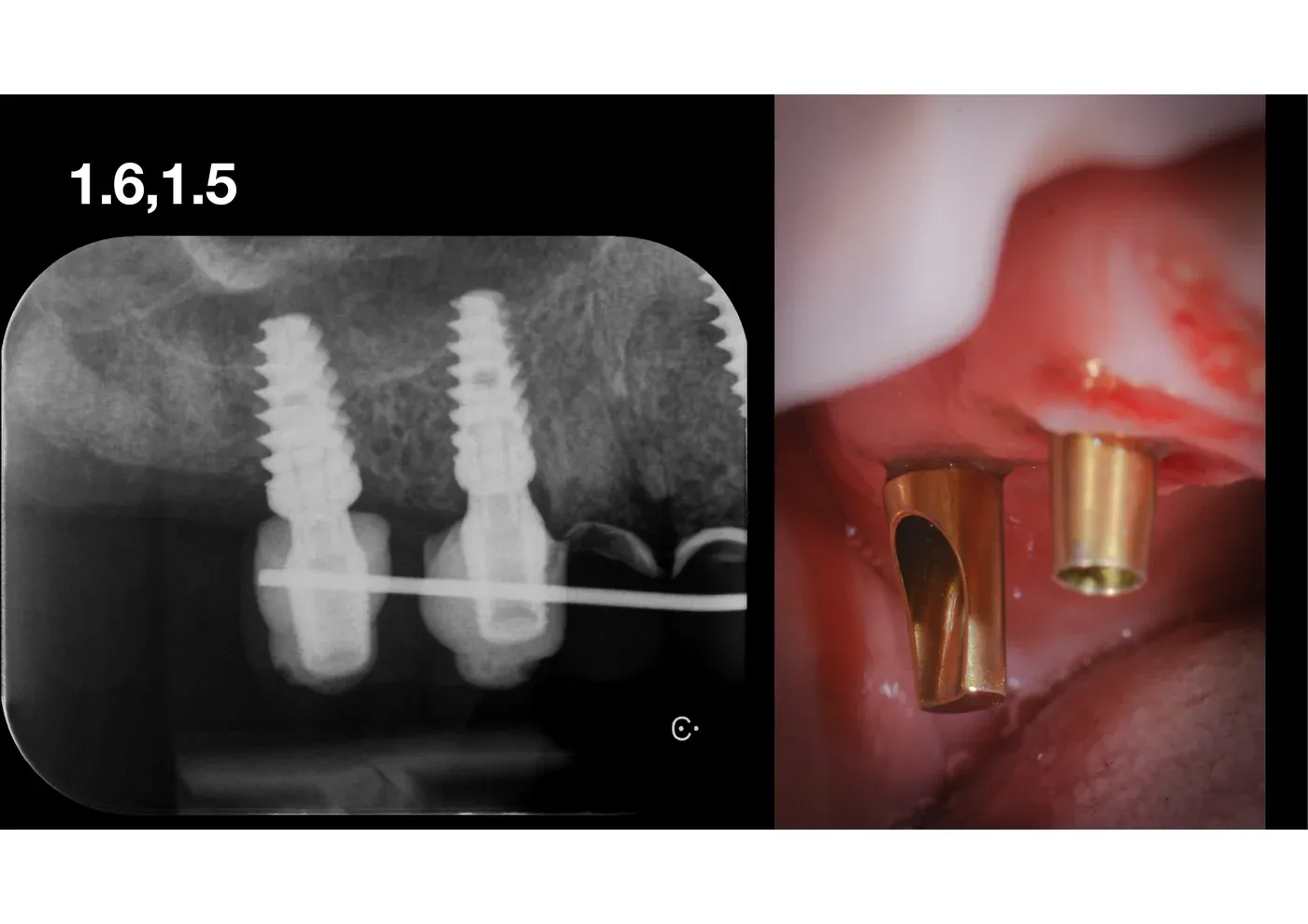
At re-entry, the radiograph shows the lift radiologically stable, the newly formed peri-apical bone (still, no graft, just from the clot) radiopaque, the implants integrated. Transition abutments (“healing screws”) are placed to shape the soft-tissue emergence profile before the definitive prosthesis.
Outcome
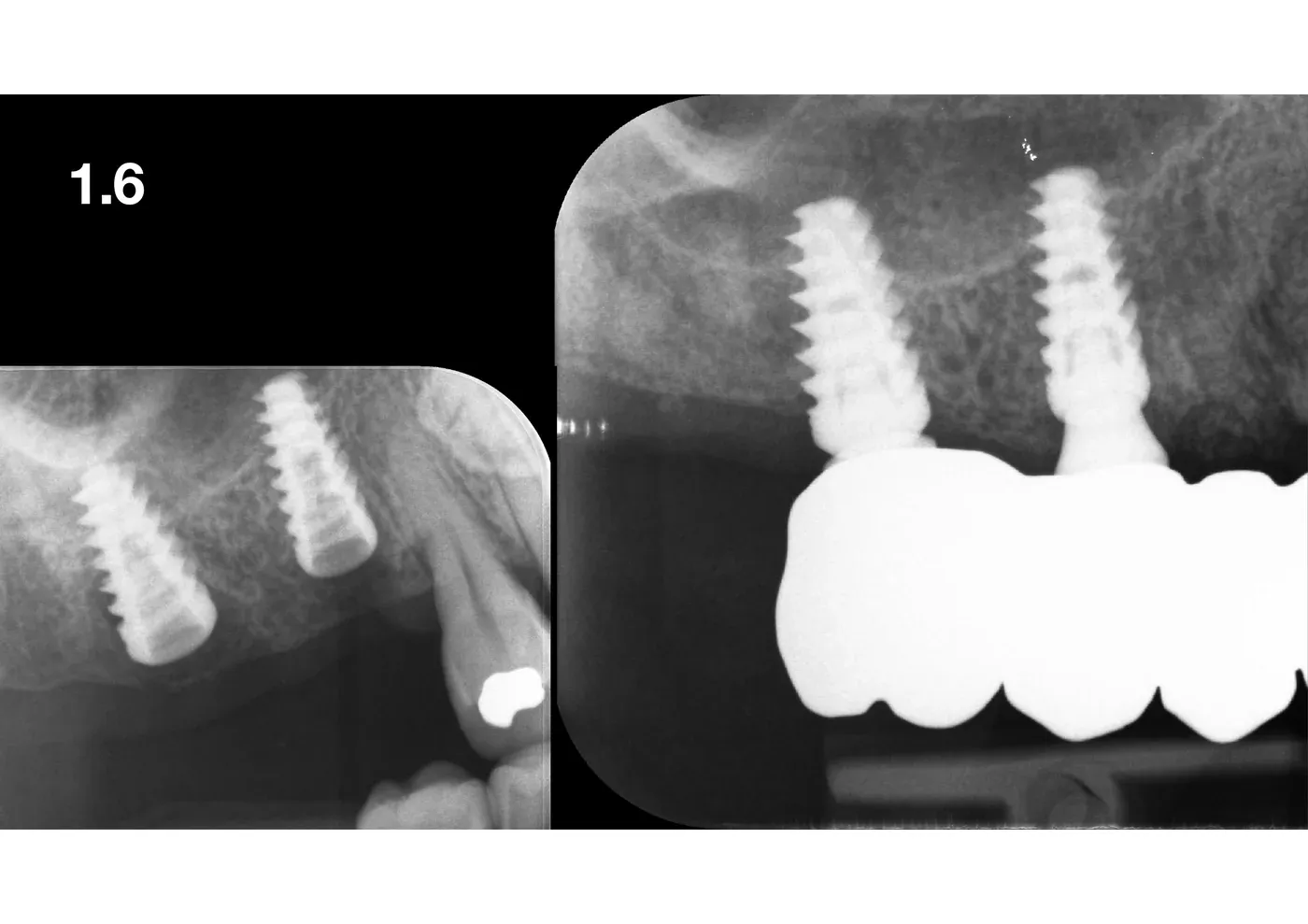
Definitive prosthetic restoration: implant-supported bridge (part of a full-arch restoration), balanced occlusion, physiological inter-proximal spaces. The final radiograph confirms stable bone levels and preservation of the lift over time.
Why graftless
Three clinical reasons. One cultural.
Biological. The blood that fills the sub-membranous space is already an osteoinductor. The lifted Schneiderian membrane, the implant apices as tent poles, the surrounding bony walls: it is the perfect environment for guided tissue regeneration. The meta-analysis by Guo and colleagues (2020) in Scientific Reports⁴ confirmed an implant survival rate of 97% at one year with non-grafted TSFE (transcrestal maxillary sinus elevation), comparable to TSFE with platelet concentrates. No significant differences. Biology did not necessarily need us.
Economic. No biomaterial means no cost of biomaterial, no carrier, no fibrin glue. For the patient it is less; for the clinician it is less to manage.
Risk. Fewer foreign bodies, less surface to be colonised, less biofilm waiting. A maxillary sinusitis after a lift is almost always a sinusitis of the biomaterial. If the biomaterial is not there, that risk drops.
Cultural. Bonebending. Displacing instead of adding. 4.0 is the sinus version of a principle the family has cultivated for over 40 years: use what is there, before importing what is not.
Indications and limits
Graftless LMSF is not universal. Especially for those with less experience, it is advisable to perform it when residual bone height is at least 4-5 mm, primary implant stability is easily achievable, the membrane is intact on CBCT, there is no active sinus pathology (pus), and the patient is not a heavy smoker or quits for healing.
It is not done when the ridge is too short to stabilise the implant, the membrane is diseased and poorly resistant, there is symptomatic sinus pathology, or the anatomy simply asks for the lateral window. Choosing the technique is, above all, a choice of respect — towards the patient and towards our wonderful work.
What the evidence says
The systematic review by Cobo-Vázquez and colleagues (2025) in the International Journal of Implant Dentistry⁵ compared osteotomes and osseodensification in crestal sinus lifting, with implant survival rates between 94.1% and 100% and bone-height gains of about 3 mm in both groups. The calibrated screw expanders I use are neither one nor the other, but lie on the same continuum: progressive, controlled expansion, without percussion. Results published on analogous instruments are reassuring.
The point, in literature, is no longer whether graftless crestal lifting works. The point is case selection and the operator’s hand.
Take-home for colleagues
LMSF is not an exotic technique. It is an Italian procedure, codified thirty years ago, with long-term data and a clear logic. Anyone who knows it only as “crestal sinus lift” underrates it: it is not just a lift, it is local and simultaneous management of the ridge, of the sinus floor cortical bone, and of implant placement in a single session.
Graftless adds a layer: less biomaterial, less cost, less risk, and a result at one year that is indistinguishable from the grafted one.
Expansion 4.0 is my latest personal tuning “by Bruschis”: screw expanders, no mallet, no particulate, one philosophical lens — bonebending. If the ridge is a candidate and the membrane is a friend, 4.0 is the shortest path between bone atrophy and the implant.
For the rationale of “post-extractive” expansion with stabilised xenograft — the other side of the coin, when graftless is not enough — see the clinical case with xenograft and fibrin glue.
References
- Bruschi GB, Scipioni A, Calesini G, Bruschi E. Localized management of sinus floor with simultaneous implant placement: a clinical report. Int J Oral Maxillofac Implants 1998;13(2):219-26. PubMed
- Scipioni A, Bruschi GB, Calesini G. The edentulous ridge expansion technique: a five-year study. Int J Periodontics Restorative Dent 1994;14(5):451-9. PubMed
- Lundgren S, Andersson S, Gualini F, Sennerby L. Bone reformation with sinus membrane elevation: a new surgical technique for maxillary sinus floor augmentation. Clin Implant Dent Relat Res 2004;6(3):165-73. PubMed
- Guo T, Gulati K, Shen Z, Han P, Fan Z. Therapeutic outcomes of non-grafted and platelet concentrations-grafted transcrestal maxillary sinus elevation (TSFE): a systematic review and meta-analysis. Sci Rep 2020;10:5935. DOI · PubMed
- Cobo-Vázquez CM, García-Rodríguez S, Colmenares-Otero ME, Sáez-Alcaide LM, Cortés-Bretón-Brinkmann J, Madrigal Martínez-Pereda C, Meniz-Garcia C. Clinical and radiographic evaluation for two crestal sinus lift techniques: osteotome versus osseodensification. A systematic review and meta-analysis. Int J Implant Dent 2025;11(1):36. DOI · PubMed
FAQ
- What is LMSF (Localised Management of Sinus Floor)?
- LMSF is a surgical technique codified by Bruschi, Scipioni, Calesini and Bruschi in 1998 in the International Journal of Oral & Maxillofacial Implants. It combines crestal expansion and localised management of the maxillary sinus floor to place implants at the same time as the lift, in ridges with residual bone height of 5-7 mm, without resorting to a lateral window.
- What does «graftless» mean in sinus lifting?
- It means elevating the cortical bone of the maxillary sinus floor and the Schneiderian membrane and placing the implant without interposing any biomaterial. The sub-membranous space, kept by the tip of the implants, fills with a blood clot and is converted into bone by the principle of healing by secondary intention. Lundgren and colleagues showed the predictability of this concept as early as 2004.
- Why do you call this procedure «Expansion 4.0»?
- Because it is the fourth evolution of the family technique. 1.0 is the Scipioni-Bruschi ERE of 1994. 2.0 is the LMSF of 1998: the same logic, applied to the sinus. 3.0 is the version with magnetodynamic percussion osteotomes. 4.0 is the contemporary synthesis: screw expanders, graftless approach, management of the immediate post-extraction case.
- When can I use graftless LMSF instead of a lateral sinus lift?
- When residual bone height under the sinus is at least 4-5 mm, the anatomy is favourable, the membrane is intact on CBCT, and sufficient primary stability of the implant can be achieved. Above 6 mm the procedure is routine; below 4 mm the margin narrows and the lateral window or a crestal lift with grafting become the safer choices.
- With graftless, what forms under the membrane?
- Bone forms. The blood trapped between the elevated cortical bone, ciliated epithelium, bony walls and implant apex coagulates, is invaded by osteoblasts and mineralises. It is the same principle as the post-extraction socket. One-year evidence shows an average gain of 2.5-3.5 mm of peri-apical bone even without grafting.
- What are the specific risks of graftless LMSF?
- Three, mainly: laceration of the Schneiderian membrane during crestal expansion; loss of the sub-membranous space if the implant does not protrude enough into the sinus; failure of primary stability, which requires giving up simultaneous placement and re-entering after healing.
References
Looking for a specialist?
Implantologia a Frosinone →Impianti dentali, carico immediato e rigenerazione ossea
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stai valutando un impianto dentale?
Ho scritto una guida in 8 capitoli che spiega tutto quello che un paziente dovrebbe sapere prima di sedersi in poltrona. Niente marketing — solo fatti, casi studio e una checklist per fare le domande giuste.
Scarica la guidaStay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment