Osteo-mucosal Expansion at Site 4.6: From Severe Defect to Definitive Crown

In brief — A patient with a long-standing bridge in the lower right molar region presents with a severe combined defect: thin concave ridge plus almost absent keratinised mucosa. With osteo-mucosal expansion (Bonebending 4.0), bone and soft tissue are rebuilt simultaneously in one surgical session. Implant placed in the same session, no graft, no membrane. At three months, the screw-retained zirconia crown is in function, with a wide band of newly regenerated keratinised mucosa.
Sommario (IT) — Un paziente con un ponte di lunga data in zona 4.6 si presenta con un difetto severo combinato: cresta sottile e concava più mucosa cheratinizzata quasi assente. Con l’espansione osteo-mucosa (Bonebending 4.0), osso e tessuti molli vengono ricostruiti contemporaneamente in una sola seduta. Impianto inserito nella stessa seduta, senza innesti né membrane. A tre mesi, la corona definitiva avvitata in zirconia è in funzione, con un’ampia banda di mucosa cheratinizzata neoformata.
The starting point
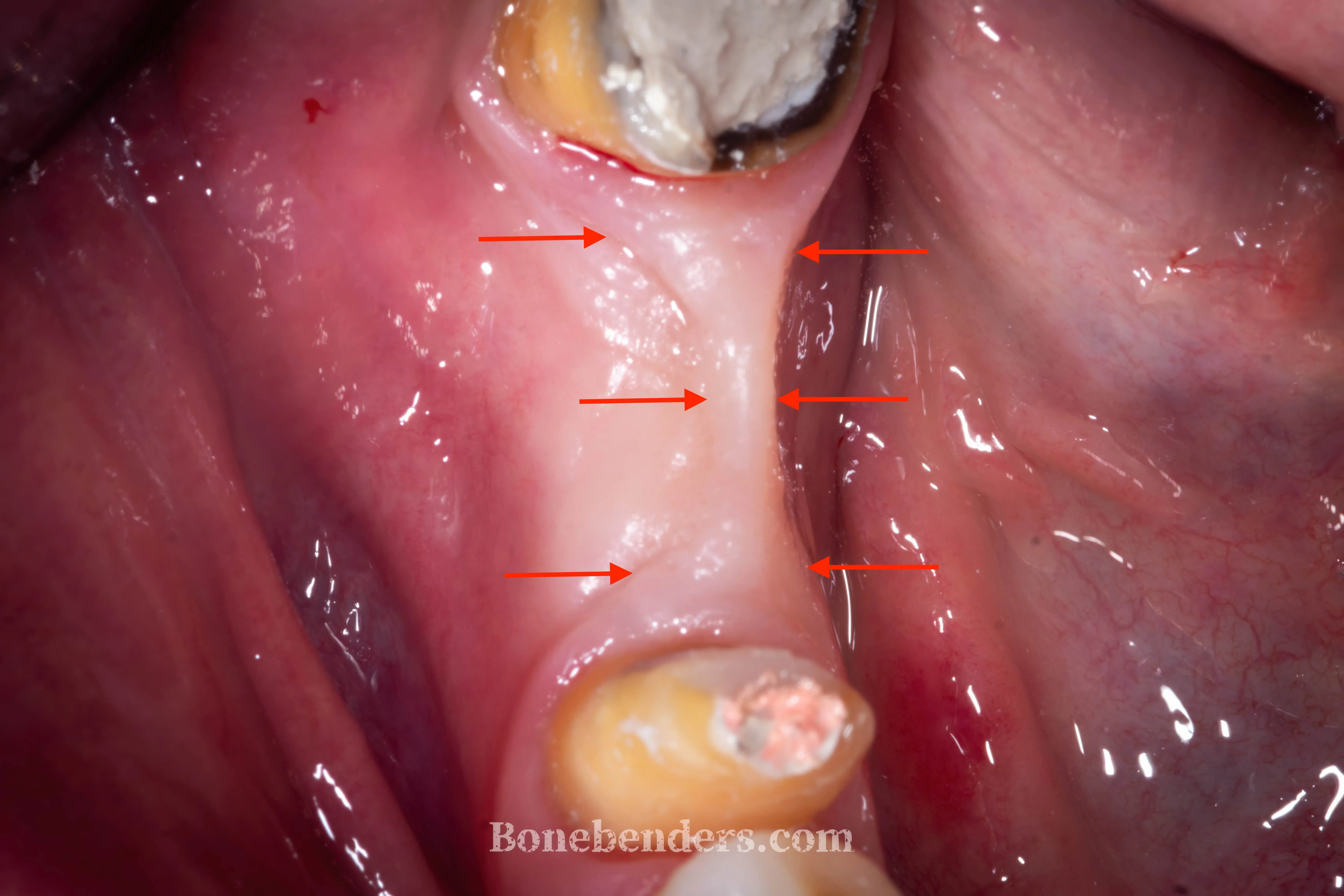
The patient presents with a single edentulous site at 4.6 (lower right first molar) with a complex picture: the ridge is concave in the bucco-lingual direction, the horizontal dimension is insufficient for conventional implant placement, and — just as importantly — the keratinised gingiva is almost absent at the edentulous site, with alveolar mucosa rising all the way to the crest.
He had been wearing a bridge for over ten years. It preserved function and aesthetics, but because of the underlying anatomical defect the pontic trapped food daily and was a constant source of discomfort and halitosis.
Hypothetically, the bridge could have been remade after a connective tissue graft. But if surgery is the chosen path, it is worth going all the way and completing the job. Together with the patient, we opted for an implant with regeneration of the defect and single crowns.
Treatment plan
In the posterior mandible, surgical choices weigh both on the functional result (high masticatory load) and on the overall rehabilitation timeline. This is one of the most demanding zones in the entire mouth — probably the area where post-extraction bone resorption strikes most aggressively, plausibly because of the kinematic torsional forces acting on the mandible and their effect on the Young’s modulus of the skeletal structure.
In this case, as in many similar ones, the plan follows the usual single-session regenerative path with minor refinements afterwards:
- Osteo-mucosal expansion (Bonebending 4.0) — the technique preserves periosteum and keratinised mucosa, working on bone and soft tissue at the same time. In a single move, displacing the bone also regenerates the keratinised mucosa.
- Simultaneous implant placement exploiting the thickness gained from the expansion.
- Cover screw with tissues approximated without tension — no membrane, no xenograft.
- Secondary intention healing of the osteo-mucosal gap: bone regenerates inside the space created, keratinised mucosa grows from the margins of the partial-thickness flap.
- Placement of a transmucosal healing screw once osseointegration is achieved, with further gain of keratinised mucosa, again by secondary intention.
- Delayed prosthetic loading after osseointegration, with a screw-retained definitive zirconia crown.
Surgery
The incision follows a partial-thickness flap design: only the deep connective tissue is dissected, leaving part of it with the periosteum still attached to the bone. This choice is critical — it is the periosteum (or, more precisely, the connective tissue adherent to the bone) that is mainly responsible for vascularisation, preservation of the bundle bone, and bone regeneration inside the empty space created by the expansion.
The longitudinal osteotomy is performed with calibrated instruments alternated with burs, and the lateral expansion proceeds progressively and rapidly until the thickness compatible with the chosen implant diameter is reached.
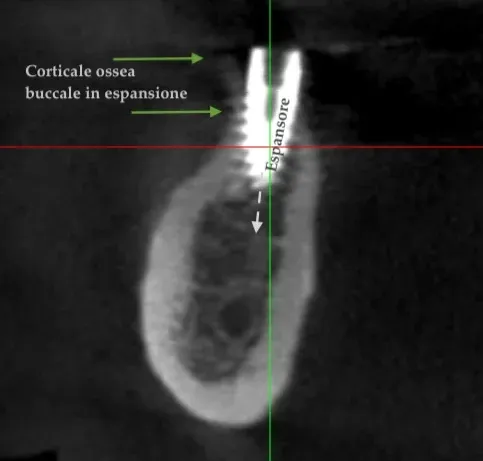
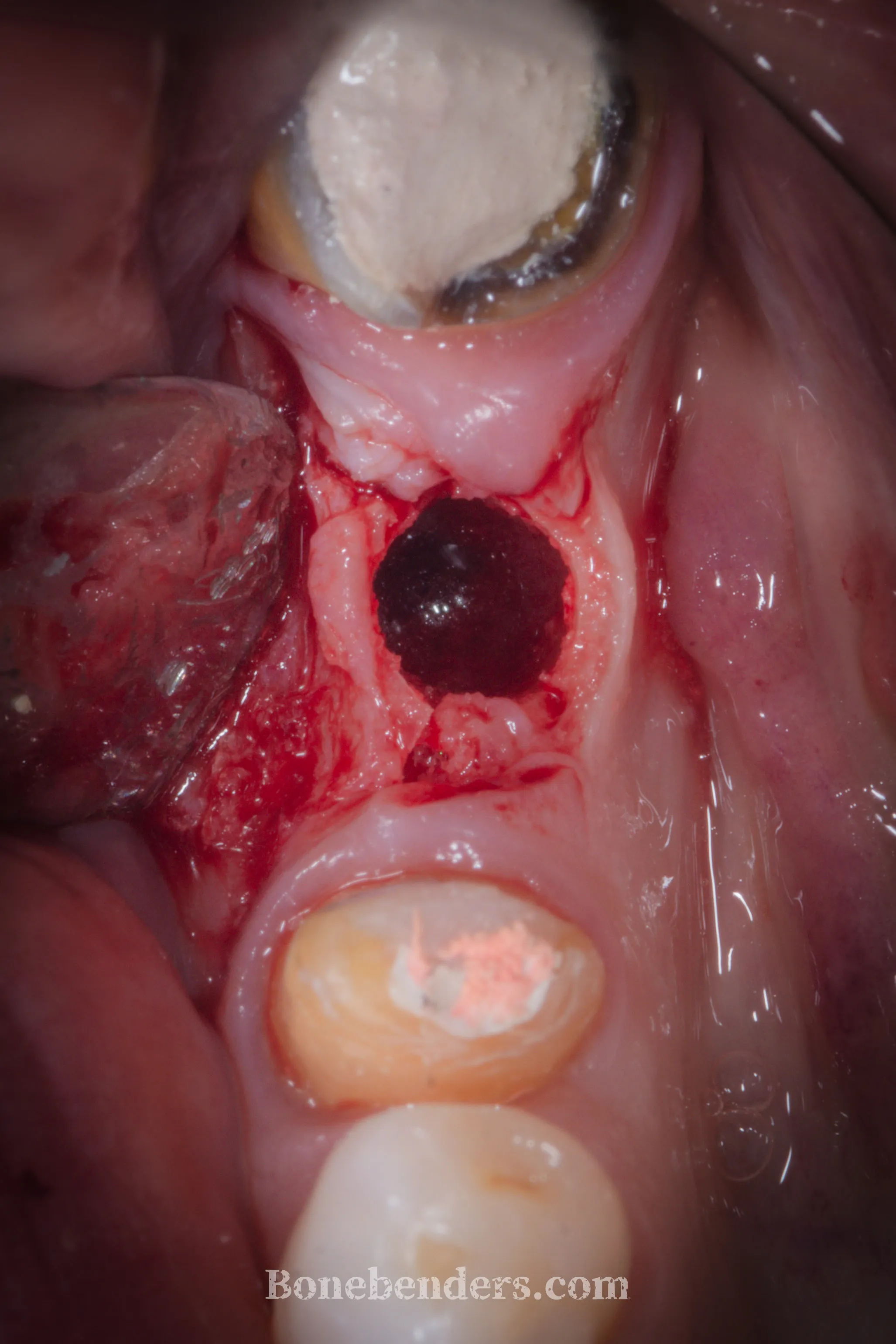
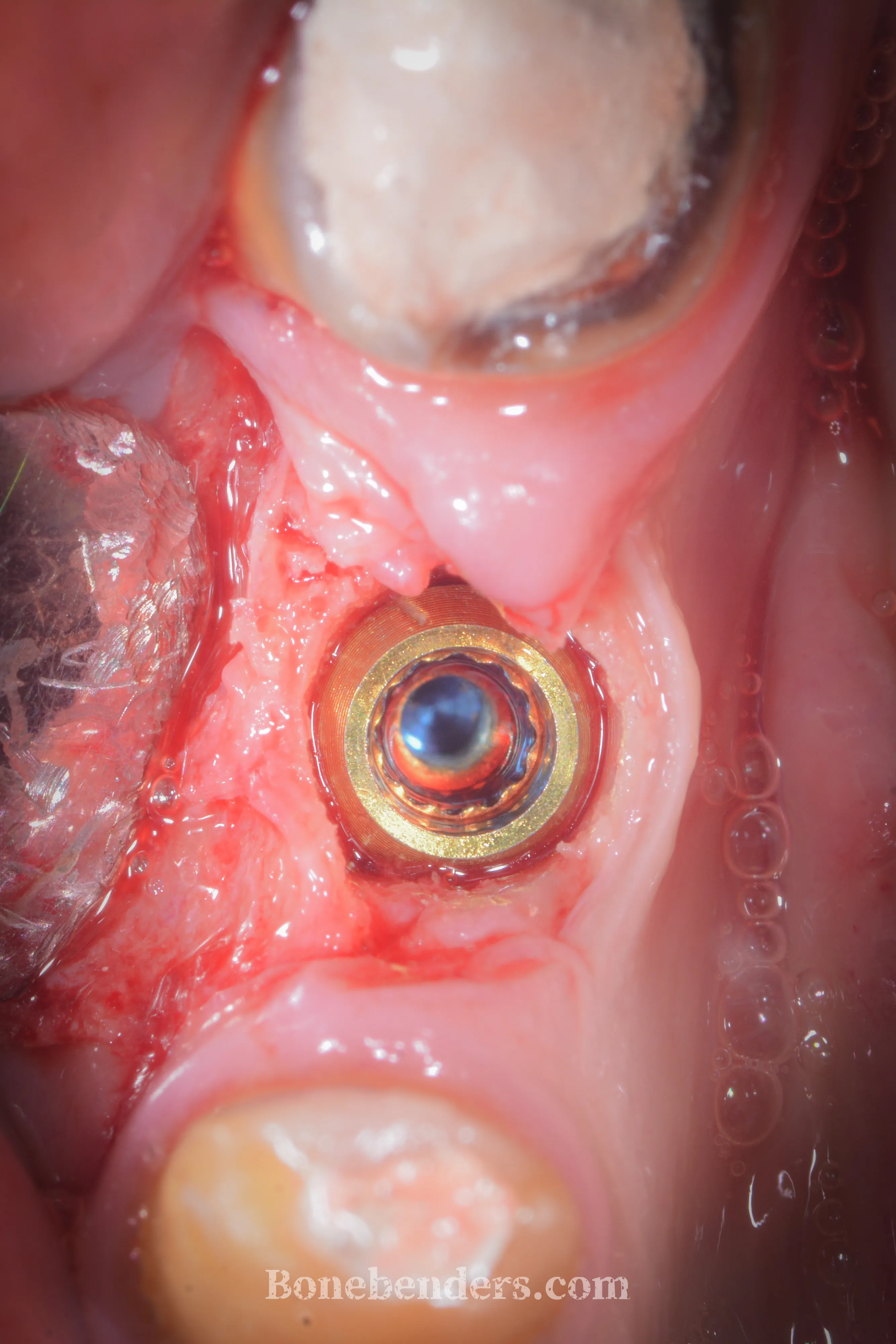
The implant is placed in the expanded site with exceptional primary stability — a point that often goes unnoticed, more for conceptual than logical reasons — and a cover screw is applied. No xenograft, no membrane: the residual gap heals by secondary intention, using the blood clot as a natural biological scaffold.
The transmucosal healing screw is then applied once osseointegration is complete, to gain further keratinised mucosa. Classical submerged healing is more favourable from this point of view.
In the images that follow, the impressive osteo-mucosal regeneration is evident. The keratinised tissue — almost non-existent at baseline — looks almost “in excess”. And all of this without grafts, thanks to secondary intention healing.


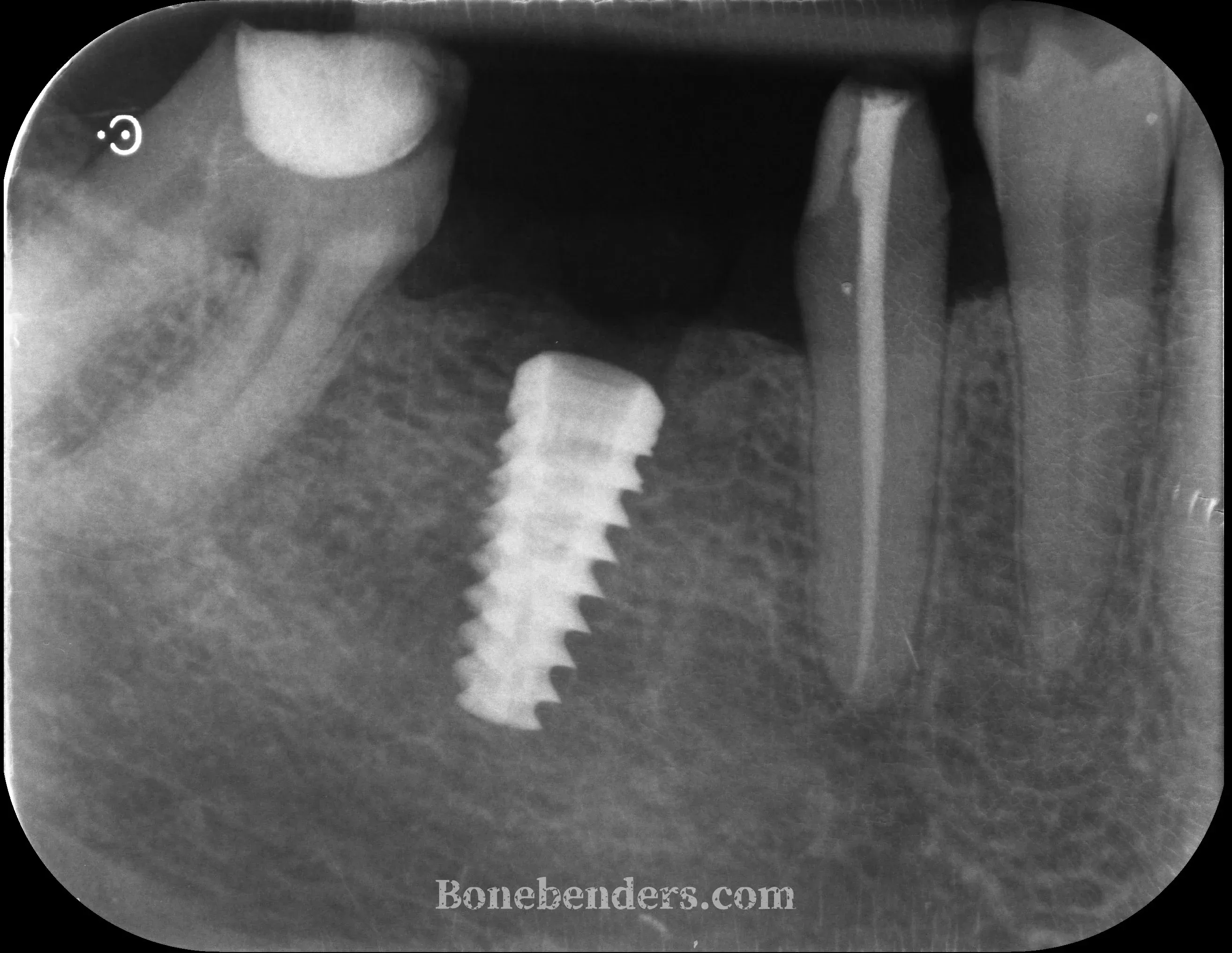
Result
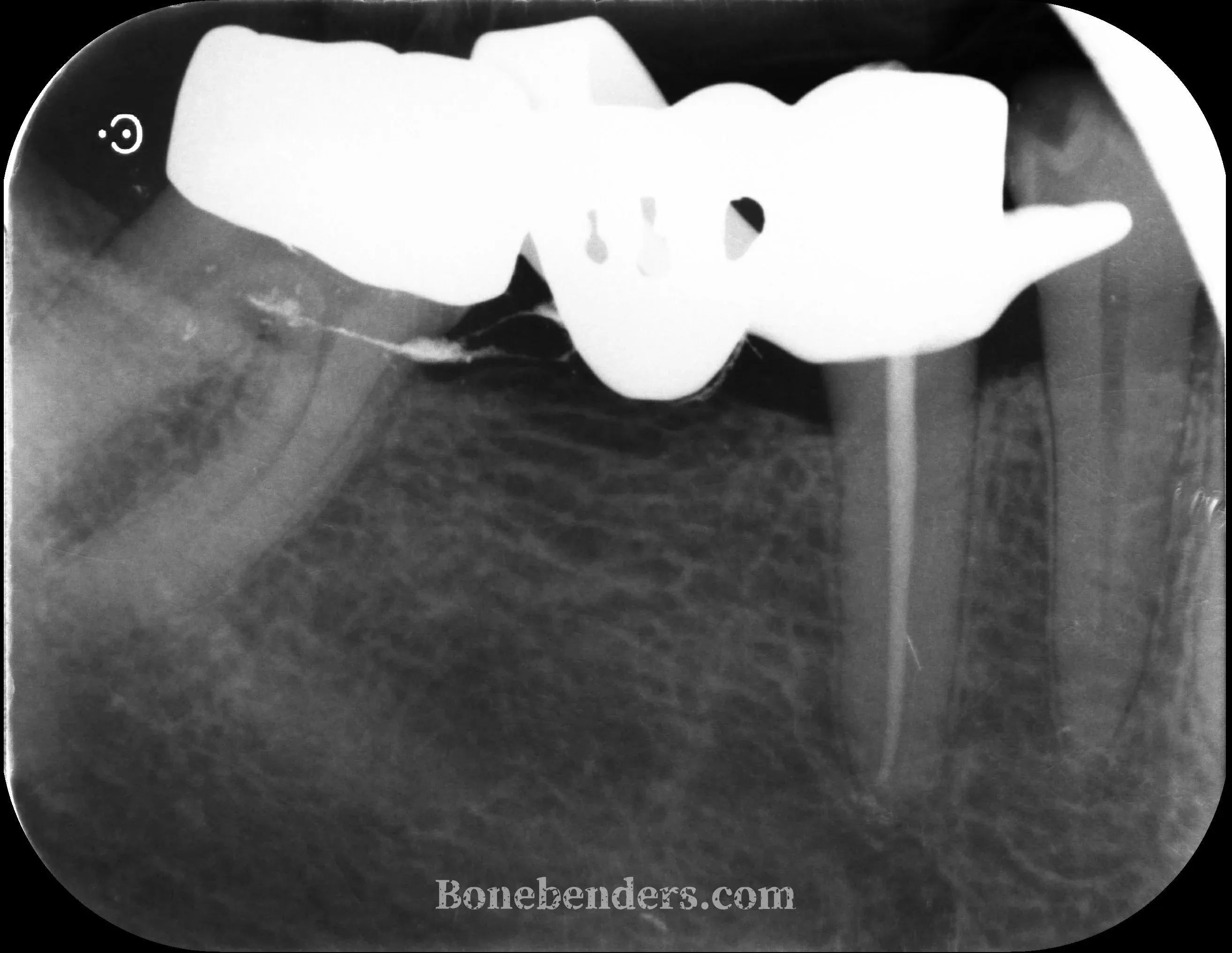
At three months from implant placement, the screw-retained definitive crown at 4.6 is in function. Early osseointegration is complete, radiographic bone levels are stable around the implant, and the soft tissues show complete aesthetic and functional integration: healthy festooned gingiva matching the colour of the adjacent teeth, with a keratinised band wide enough to ensure long-term peri-implant stability.
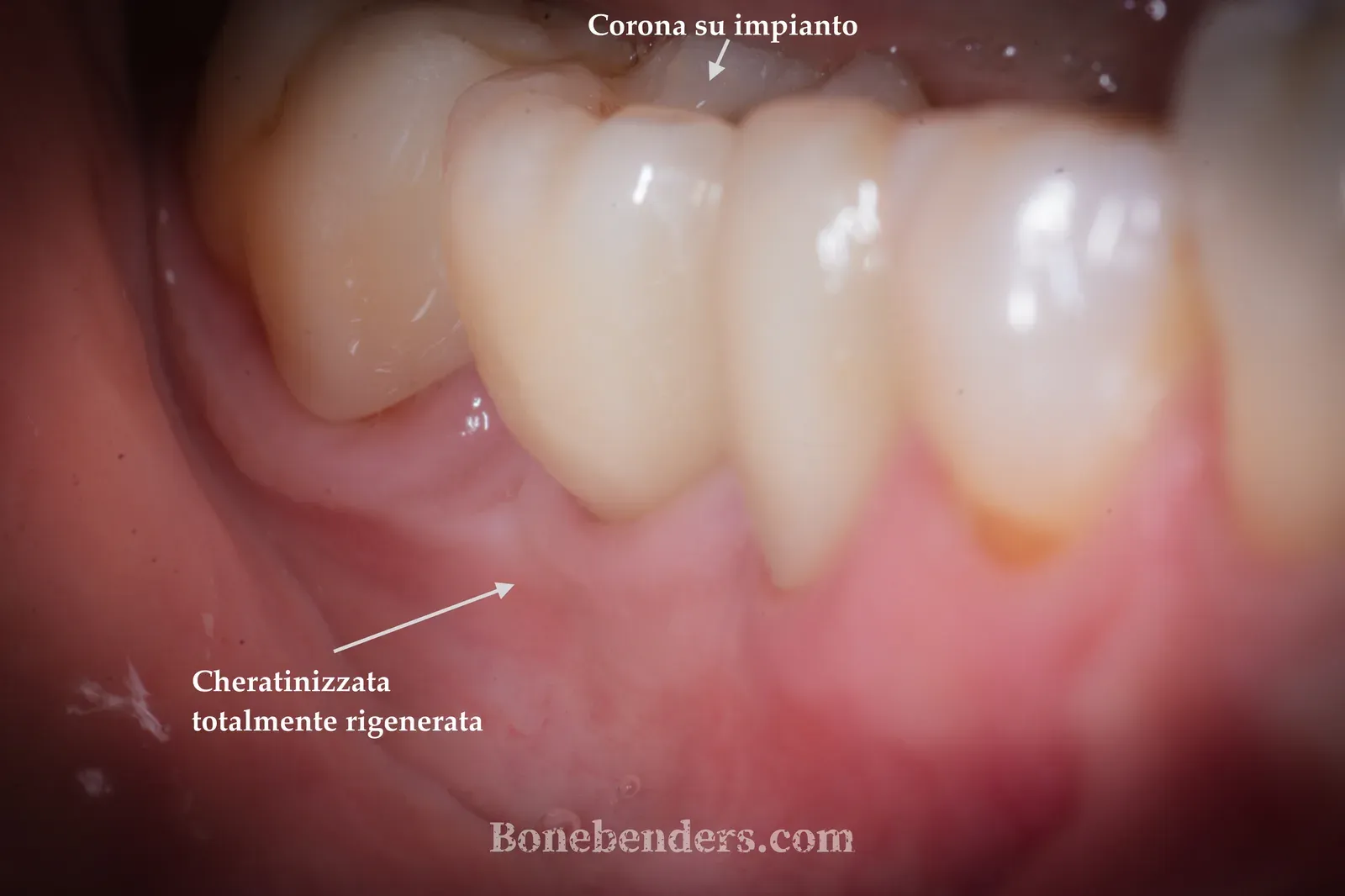

Peri-implant probing is physiological on every aspect, with no bleeding. The patient reports full masticatory function and no sensitivity at the site. The case shows how, in experienced hands and with the correct pre-operative assessment, osteo-mucosal expansion makes it possible to manage in a single surgical session defects that with traditional techniques would have required two stages and substantially longer healing times.
Frequently Asked Questions
What is osteo-mucosal expansion (Bonebending 4.0)?
It is an evolution of the ERE split-crest technique that works in a single surgical session on bone and soft tissue together. Instead of raising a full-thickness flap — which would strip the bone of its periosteum and the soft tissue of its vascularisation — a partial-thickness flap is elevated, and an osteotomy is performed that allows lateral expansion of the ridge while preserving both the vascular supply and the keratinised mucosa.
Why was a bone graft avoided?
Bone regenerates by secondary intention inside the gap created by the expansion, using the patient’s own blood as a natural biological scaffold. The intact periosteum is essential to this process. Avoiding a xenograft means zero infectious risk associated with the biomaterial, faster healing times, and no additional cost to the patient.
Could the same result have been achieved with other techniques?
The classical alternatives for such an atrophic ridge are guided bone regeneration (GBR) with a membrane or an autologous block graft. Both require longer timelines (4–6 months of waiting before implant placement), higher risks of exposure or infection, and — for autologous harvest — a second surgical site. When the defect involves the soft tissue as well, as in this case, osteo-mucosal expansion is particularly advantageous because it rebuilds bone and keratinised mucosa simultaneously.
Further reading
- ERE expansion and immediate implant: a premolar in one session
- Bone remodelling: the cycle that decides the life of implants
- Regeneration without harvesting: the biology of graftless healing
Sources
- Bruschi GB, Scipioni A et al. (1998) — Int J Oral Maxillofac Implants — PMID 10635173 — Localized management of sinus floor with simultaneous implant placement
FAQ
- What is osteo-mucosal expansion (Bonebending 4.0)?
- It is an evolution of the ERE split-crest technique that works in a single surgical session on bone and soft tissue together. Instead of raising a full-thickness flap — which would strip the bone of its periosteum and the soft tissue of its vascularisation and elasticity — a partial-thickness flap is elevated, and an osteotomy is performed that allows lateral expansion of the ridge while preserving both the vascular supply and the keratinised mucosa.
- Why was a bone graft avoided?
- Bone regenerates by secondary intention inside the gap created by the expansion, using the patient's own blood and cells as a natural biological scaffold. The intact periosteum is essential to this process. Avoiding a xenograft means zero infectious risk associated with the biomaterial, faster healing times and no additional cost to the patient.
- Could the same result have been achieved with other techniques?
- The classical alternatives for such an atrophic ridge are guided bone regeneration (GBR) with a membrane or an autologous block graft. Both require longer timelines (4–6 months of waiting before implant placement), higher risks of exposure or infection, and — in the case of autologous harvest — a second surgical site. When the defect involves the soft tissue as well, as in this case, osteo-mucosal expansion is particularly advantageous because it rebuilds bone and keratinised mucosa simultaneously.
References
Looking for a specialist?
Implantologia a Frosinone →Impianti dentali, carico immediato e rigenerazione ossea
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stai valutando un impianto dentale?
Ho scritto una guida in 8 capitoli che spiega tutto quello che un paziente dovrebbe sapere prima di sedersi in poltrona. Niente marketing — solo fatti, casi studio e una checklist per fare le domande giuste.
Scarica la guidaStay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment