Immediate Implant Placement Is (Almost) Always the Best Solution
In brief — Immediate implant placement is nearly always the best option to replace an extracted tooth, regardless of the bone defect. The only true contraindication is acute infection. Alveolar defects, including buccal plate loss and pneumatised sinuses, can be corrected during implant placement with excellent primary stability.
The philosophy: competence and courage
Oral surgeons and periodontists who place implants must be careful, but they must also be competent.
In the end, you have to be yourself.
I am myself when I offer my patients the best possible treatment, safely.
I am myself when I do not follow common trends.
I am myself when my treatment is in line with the patient’s expectations, and is at the same time the fastest and least invasive option available.
I firmly believe that an immediate implant is always the best solution when a tooth is not treatable.
The only true contraindication is acute infection.
In the vast majority of cases, alveolar bone defects of any kind — including buccal defects caused by infection, and heavily pneumatised maxillary sinuses requiring lift — can be corrected successfully during implant placement.
This is not just my clinical impression. A 2025 systematic review with meta-analysis by Campi and colleagues in Quintessence International pooled five randomised controlled trials on implants placed in “damaged” sockets — with buccal wall loss, residual infection, alveolar bone defects. Implant survival: 100%. Pink Esthetic Score equivalent to intact sites. No significant differences in marginal bone loss compared with healed sites. The condition — the authors stress — is concurrent bone regeneration and rigorous adherence to protocol. Exactly what I have been doing for years.
I can say this with confidence, because I have successfully treated hundreds of cases with this protocol.
The vast majority of these cases were immediately restored with a temporary prosthesis to preserve the patient’s aesthetics. In some cases, the implants need a short healing period before they can be loaded. Implant stability is the deciding factor between immediate loading and delayed loading — and on this point, the implant design itself matters a great deal.
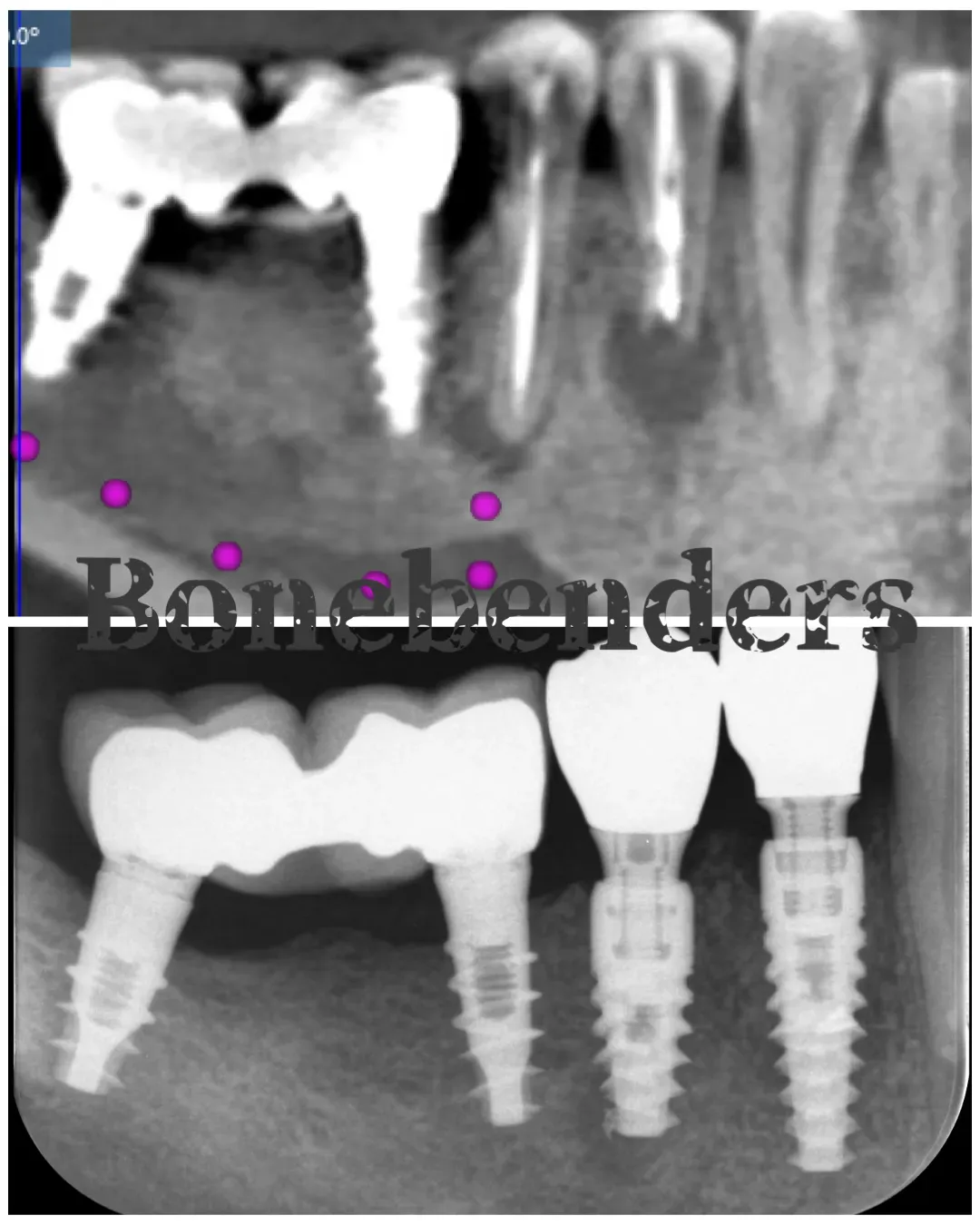
The clinical case: lower premolars with buccal defect
A typical case is shown here. The two right lower premolars of this 60-year-old ASA 1 patient presented with recurrent abscesses. I discussed the treatment options with him and we decided together to proceed with extractions, immediate implants and provisional restorations.
The first premolar had completely lost its buccal bone wall, as shown by the CBCT cross-section below.
To achieve sufficient primary stability in a case like this, the apical portion of the implant must engage the healthy, stable basal bone below the lesion. If the implant is properly designed, the apical portion will provide the stability the system needs throughout osseointegration, while also achieving contact osseointegration on the threads already engaged in basal bone and, over time, distance osseointegration in the areas initially devoid of osteons.
Naturally, bone defects must be grafted with osteoconductive biomaterial (or, alternatively, autologous bone harvested from the same patient) to reduce tissue volume loss and recreate the alveolar process architecture in the medium-to-long term.
In this case, primary stability of both implants was excellent, allowing the placement of an immediate provisional prosthesis. Using a flapless “through-the-socket” approach, I grafted the buccal defect with a simple heterologous bone xenograft. This is, quite simply, the best way to graft: no flaps when possible.
The 2025 meta-analysis by Mansouri and colleagues in Clinical and Experimental Dental Research — five RCTs, 179 implants — quantifies the benefit of contextual grafting of the peri-implant gap in flapless protocols: at 4–5 mm apical to the crest, horizontal bone preservation is significantly better when the gap is grafted (WMD 0.48 mm, favouring grafting). The number is not enormous on paper. But in vivo, on a buccal wall that already starts thin or absent, that is the difference between a stable margin and a migrating one.
As a consequence of this minimally invasive approach, patients usually experience very little discomfort. This patient, for example, took 2 grams of amoxicillin (always indicated for implant surgery) two hours before the appointment and only 1 g of paracetamol afterwards.
The image below shows the peri-implant tissues before the final intraoral scan for the ceramic crowns.

Tissue volume is well preserved even on the buccal aspect of the first premolar, where the buccal alveolar bone was totally absent at the time of extraction and implant placement.
This may go against many rules, but rules are made to be broken. And personally, I do not mind breaking the rules.
The 2024 systematic review by Martins and colleagues in Advances in Clinical and Experimental Medicine — twelve studies on the anterior aesthetic zone with deficient or missing buccal plate — converges on the same point: immediate implant placement with immediate restoration delivers acceptable aesthetic outcomes regardless of defect extension, provided you know what you are doing. The same picture emerges from the meta-analysis by Wu, Shi and Yan (2023, Int J Oral Maxillofac Implants) on 421 patients: 97.8% implant survival, midfacial recession contained at 0.33 mm at one year and 0.54 mm at five years. The message is not “feasible in selected cases”. It is: predictable, when primary stability is excellent and grafting is done well.
Let me emphasise once again that the best implant is an immediate implant, which is feasible in most cases.

The final result
The contours of the final ceramic crowns are natural and the dimensions of the keratinised mucosa are optimally preserved — to the benefit of the long-term health of the implants.

The final periapical radiograph shows the implants and grafts integrated perfectly. Note how the apical granuloma of the second premolar healed cleanly at the implant apex. The granuloma was not removed. In fact, no granulation tissue should ever be removed (except in the presence of purulence and debris that cannot otherwise be cleared). That habit is a leftover from distant eras and from a “mechanistic” view of oral surgery — it has no scientific foundation.
References
-
Campi M, Leitão-Almeida B, Pereira M, Shibli JA, Levin L, Fernandes JCH, Fernandes GVO, Borges T. Immediate implant placement in damaged extraction sockets: a systematic review and meta-analysis of randomized controlled trials. Quintessence Int. 2025;56(1):34-45. doi:10.3290/j.qi.b5768294. PMID: 39351790.
-
Mansouri SS, Musaie F, Mirzaei A, Samadizadeh S, Salmasi SC, Bitaraf T. Flapless Immediate Implant Placement With and Without Bone Grafting: A Systematic Review and Meta-Analysis. Clin Exp Dent Res. 2025;11(4):e70182. doi:10.1002/cre2.70182. PMID: 40700624.
-
Martins SCR, Marques MDC, Vidal MG, Tolentino PHMP, Dinelli RG, Fernandes GVO, Shibli JA. Is the facial bone wall critical to achieving esthetic outcomes in immediate implant placement with immediate restoration? A systematic review. Adv Clin Exp Med. 2024;33(9):979-997. doi:10.17219/acem/173573. PMID: 38180330.
-
Wu XY, Shi JY, Yan Q. Midfacial Soft Tissue Recession Following Immediate Implant Placement with Bone Grafting in the Esthetic Area: A Systematic Review and Meta-analysis. Int J Oral Maxillofac Implants. 2023;38(2):239-250. doi:10.11607/jomi.10014. PMID: 37083916.
FAQ
Can an immediate implant be placed even with severe buccal bone defects?
How is tissue volume preserved in extensive buccal defects?
When is immediate loading indicated versus delayed loading?
What is the psychological advantage of immediate over delayed loading?
References
- https://doi.org/10.3290/j.qi.b5768294
- https://doi.org/10.1002/cre2.70182
- https://doi.org/10.17219/acem/173573
- https://doi.org/10.11607/jomi.10014
- https://pubmed.ncbi.nlm.nih.gov/39351790/
- https://pubmed.ncbi.nlm.nih.gov/40700624/
- https://pubmed.ncbi.nlm.nih.gov/38180330/
- https://pubmed.ncbi.nlm.nih.gov/37083916/
Looking for a specialist?
Implantologia a Frosinone →Impianti dentali, carico immediato e rigenerazione ossea
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stai valutando un impianto dentale?
Ho scritto una guida in 8 capitoli che spiega tutto quello che un paziente dovrebbe sapere prima di sedersi in poltrona. Niente marketing — solo fatti, casi studio e una checklist per fare le domande giuste.
Scarica la guidaStay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment