The Migrant Bacterium — JP2, the African Aggressor

In brief — The JP2 genotype of Aggregatibacter actinomycetemcomitans originated in Africa and spread globally through human migration. Linked to an aggressive form of periodontitis that rapidly destroys molars and incisors, especially in young people of African descent, the bacterium keeps a distinct tropism for its populations of origin — and a remarkable talent for disarming the immune system.
The origin
The JP2 genotype of Aggregatibacter actinomycetemcomitans (Aa) is widespread in Morocco and Ghana, where it is found in high percentages. This particular bacterial variant has been linked to aggressive forms of periodontal disease, making its presence an important risk factor for the oral health of local populations.
In particular, as we’ll see further on, this periopathogen is strikingly aggressive toward the young — children and adolescents included.

It has spread to other continents over millennia too, probably through the slave trade, which would have facilitated the interpersonal exchange of pathogens and disease.
Beyond the two African countries mentioned, the axis of this genotype can be traced across several ethnic groups, contributing to a broader understanding of its epidemiology and its impact on public health worldwide.
The molar-incisor axis
There is a particularly insidious form of periodontal disease that mainly affects molars and incisors, very often associated with the presence of our Aggregatibacter actinomycetemcomitans.
It was originally called juvenile periodontitis, but since we love holding workshops to change classifications and definitions (for the better, one hopes), it became aggressive periodontitis and, since 2017, periodontitis with a molar-incisor pattern.
The latest definition does, in fact, capture its main feature efficiently, and it speaks intuitively even to those who were distracted during lectures — making the recognition of the disease, and the right therapy, more inclusive and accessible.
It isn’t only a matter of names. A 2026 study in the Journal of Periodontal Research (Stolf and colleagues) sequenced the subgingival biofilm with shotgun metagenomics and found something subtle: the molar-incisor form and the generalized form of grade C, though they carry the same label, have different microbial signatures. Aggregatibacter actinomycetemcomitans stands out precisely in the molar-incisor pattern; in the generalized picture the red-complex pathogens dominate instead — Porphyromonas gingivalis, Tannerella forsythia, Treponema denticola — alongside higher levels of interleukins. Two diseases under the same surname, in short. Which gives new meaning to the whole nosographic struggle, from the old word juvenile to the 2017 classification: we weren’t just changing words, we were separating two biologies.
Let’s look at radiographs characteristic of this condition (image copyright Miguel and Shaddox, 2024 - CC4.0 license).
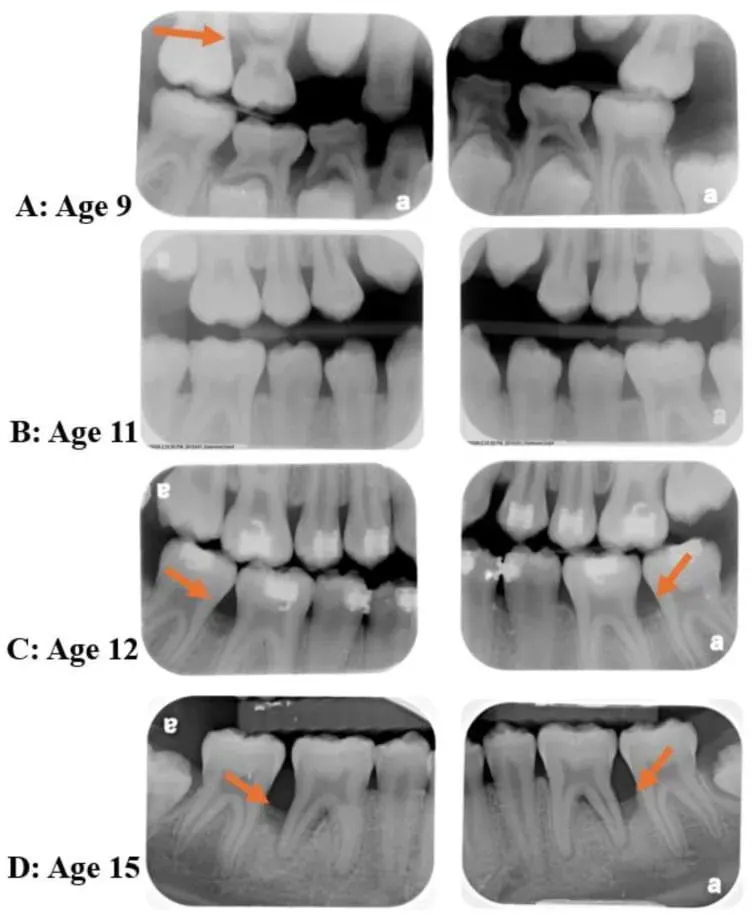
From these radiographs of a very young person, followed from ages 9 to 15, you can see the severe and extensive destruction of the alveolar bone, particularly at the molar sites (red arrows).
Recently, I examined a slightly less young person, with the serious consequences this disease can cause.
This person had no symptoms at all. The only thing they had noticed lately was a recession of the soft tissues on the lower incisors.
During the visit, everything became very clear: the molar-incisor pattern, the clinical history, and the insufficient therapies.
The easy-screw syndrome
Before reaching my observation, this person had been offered the extraction of the most compromised teeth, to replace them with implants. Yet this approach ignores the diagnostic aspects that matter for avoiding relapse, and the curative needs aimed specifically at this kind of disease.
In this case, the first step was a combined treatment of local decontamination under regional anesthesia (root planing) and targeted antibiotic therapy. Afterward, we’ll do our best to save the teeth, with regenerative periodontal surgery.
That decontamination comes before extraction is not a whim of the workshop. In a 2025 randomized trial in Clinical Oral Investigations, Paşalı and colleagues showed that, in stage III/IV grade C periodontitis, non-surgical therapy spread over three sessions lowers red- and orange-complex pathogens and inflammatory markers more than a single session — at the same clinical outcome. Translated: how you remove the biofilm matters as much as whether you do. And the shiny shortcuts deserve suspicion. Another randomized trial, from 2026 in BMC Oral Health (Cetiner and colleagues), added gaseous ozone to non-surgical therapy in grade C molar-incisor patients: the only measurable advantage was a drop in interleukin-8, with no clinical or microbiological benefit beyond plain old instrumentation. First you decontaminate well, then you decide what to extract. For the more advanced forms, I’ve described elsewhere how severe periodontitis is treated.
That strange affinity for populations of origin
JP2 is present in highly variable percentages across populations worldwide.
We know there is a substantial difference between those who have periodontal disease and those who don’t. Within the same population, the percentage of individuals carrying this periopathogen in their oral biofilm can be very low in healthy subjects and very high in those who, instead, have a confirmed diagnosis of periodontitis.
In some Asian populations, JP2 prevalence is very high even in healthy subjects (provided they really are healthy, and not misdiagnosed).


It is certain that this bacterial genotype has kept a high tropism for its populations of origin, whose peculiar anthropological and genetic features evidently favor its proliferation. And so in the Scandinavian countries, for example, ours spreads far more among subjects of North African origin than in the general population.
The aggression against the immune system
Like all Aa strains, JP2 too causes periodontitis in young people and adolescents with the classic molar-incisor pattern. And it stands out for its extremely strong aggressive capacity against leukocytes, and therefore against the immune system.
Specifically, the JP2 genotype is characterized by significantly higher leukotoxin production than other genotypes. This elevated leukotoxin output generates a greatly increased pathogenic potential, making carriers more vulnerable to severe periodontal disease.
But the damage isn’t only a matter of how much toxin. In 2026, in Scientific Reports, Khoury and colleagues challenged oral neutrophils ex vivo with the JP2 strain itself: in patients with the molar-incisor pattern, those white cells produced less reactive oxygen species and responded with an altered cytokine profile compared with healthy subjects. It’s a detail worth pausing on. JP2 doesn’t simply kill leukocytes: it reprograms their response, leaves them disoriented, and in the meantime the bone is left exposed. And the matter doesn’t stop in the mouth. A 2026 review in the Journal of Oral Microbiology (Seguel-Fuentes and colleagues) reconstructs how leukotoxin A, LPS and the cytolethal distending toxin travel packaged in outer-membrane vesicles all the way to distant tissues, fueling a systemic inflammation that has been associated even with rheumatoid arthritis. A bacterium that starts in the gingival sulcus and ends up talking to the joints.
In conclusion
It is believed that the JP2 clone of Aggregatibacter actinomycetemcomitans, strongly associated with aggressive periodontitis in adolescents of African origin, arose in the Mediterranean part of Africa about 2,400 years ago. It then spread to West Africa and was later transferred across the American continents during the slave trade. The clone has kept a distinct tropism for its original host, predominantly colonizing individuals of African origin despite centuries of geographic separation.
A very interesting study also suggests intrafamilial transmission, supporting the idea that the spread of the JP2 clone was initially confined to close contacts.
References
- Stolf CS, Paz HES, Paraluppi MC, et al. Molar-Incisor and Generalized Grade C Periodontitis: Distinct Microbiome-Immune Interactions Suggest Divergent Pathogenesis. J Periodontal Res. 2026;61(4):382-395. doi:10.1111/jre.70077 · PMID: 41664846
- Khoury J, Haloun B, Musai N, et al. Distinct functional profiles of oral neutrophils in molar incisor pattern periodontitis, generalized periodontitis and periodontal health. Sci Rep. 2026;16(1):12641. doi:10.1038/s41598-026-39112-3 · PMID: 41796124
- Paşalı Ç, Emingil G, Yılmaz B, Kantarcı A. Three-session non-surgical therapy stabilizes microbiological and biochemical responses in patients with stage III/IV grade C periodontitis: a randomized clinical trial. Clin Oral Investig. 2025;30(1):29. doi:10.1007/s00784-025-06724-4 · PMID: 41449292
- Cetiner DO, Karaduman B, Selman AE, Gonen S, Corekci AU. Adjunctive effect of gaseous ozone on inflammatory biomarkers and microbial profile in grade C molar-incisor pattern periodontitis: a randomized split-mouth placebo-controlled clinical trial. BMC Oral Health. 2026;26(1):938. doi:10.1186/s12903-026-08213-w · PMID: 41942979
- Seguel-Fuentes E, Quidel B, García-Pissani B, et al. Aggregatibacter actinomycetemcomitans virulence factors and systemic inflammation: linking periodontitis to rheumatoid arthritis. J Oral Microbiol. 2026;18(1):2647515. doi:10.1080/20002297.2026.2647515 · PMID: 41878157
FAQ
What is the JP2 genotype of Aggregatibacter actinomycetemcomitans?
Is aggressive periodontitis curable?
Why does JP2 have an "affinity" for African populations?
How is JP2 transmitted?
What are the clinical signs of molar-incisor pattern periodontitis?
References
- PubMed 37763046
- https://doi.org/10.1111/jre.70077
- https://doi.org/10.1038/s41598-026-39112-3
- https://doi.org/10.1186/s12903-026-08213-w
- https://doi.org/10.1007/s00784-025-06724-4
- https://doi.org/10.1080/20002297.2026.2647515
- https://pubmed.ncbi.nlm.nih.gov/37763046/
- https://pubmed.ncbi.nlm.nih.gov/41664846/
- https://pubmed.ncbi.nlm.nih.gov/41796124/
- https://pubmed.ncbi.nlm.nih.gov/41449292/
- https://pubmed.ncbi.nlm.nih.gov/41942979/
- https://pubmed.ncbi.nlm.nih.gov/41878157/
Looking for a specialist?
Parodontologia a Frosinone →Diagnosi e trattamento della parodontite nello Studio Denti Più
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment