Zone A and Zone B: The Histology of the Peri-Implant Biological Seal
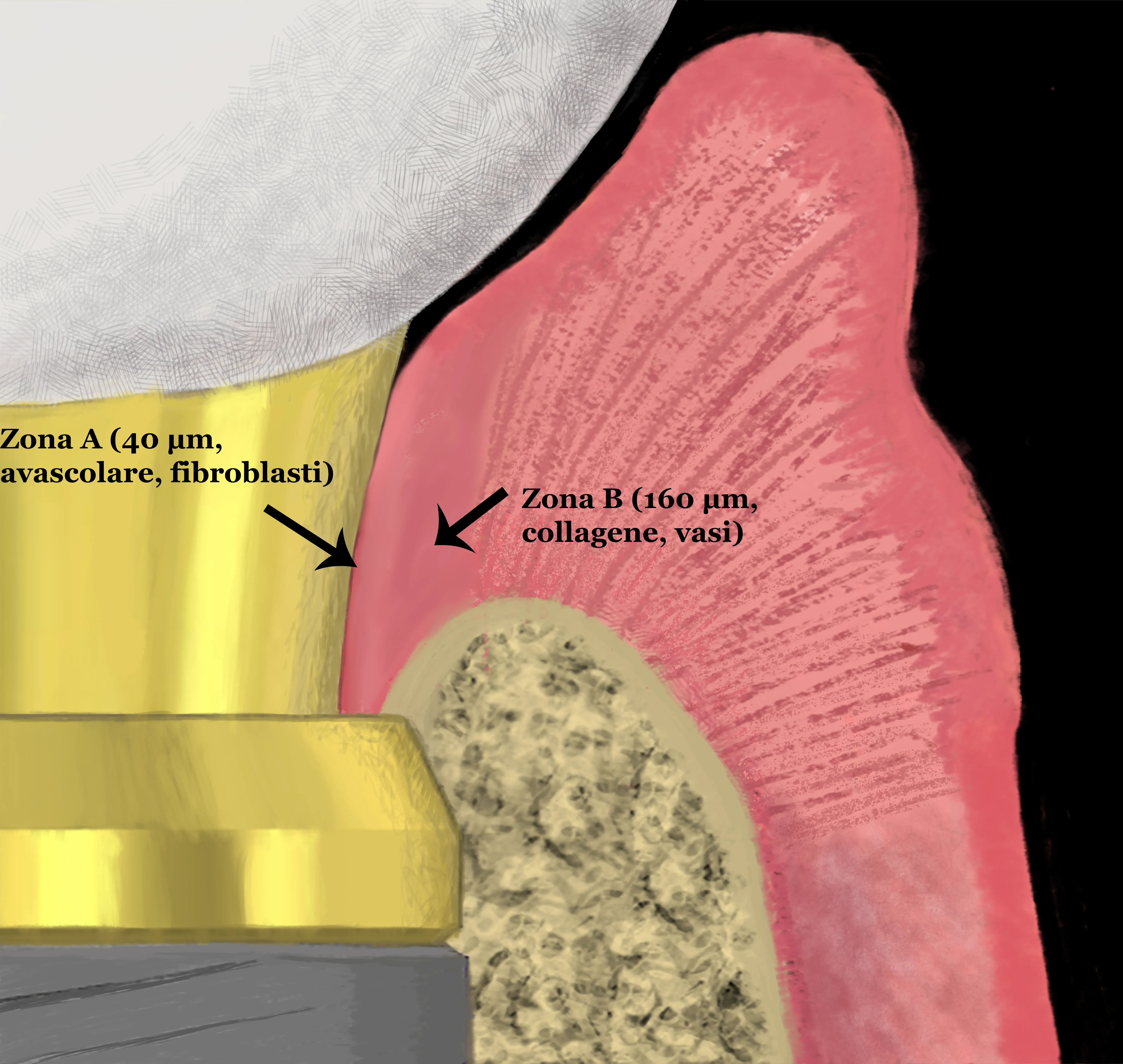
In breve — Il tessuto connettivo che circonda il collo di ogni impianto è organizzato in due zone funzionalmente distinte: Zona A (40 μm adiacenti al titanio, avascolare, ricca di fibroblasti) e Zona B (160 μm laterali, collagenosa, vascolarizzata). Moon e colleghi lo dimostrarono nel 1999 su sei beagle. La Zona A è il sigillo biologico — non una metafora. La sua integrità dipende dallo spessore mucoso, dalla cheratinizzata disponibile, e dal rispetto chirurgico del tessuto molle.
Summary (EN) — The connective tissue surrounding every implant neck is organized in two distinct functional zones: Zone A (40 μm adjacent to titanium, avascular, fibroblast-rich) and Zone B (160 μm lateral, collagenous, vascularized). Moon et al. established this histologically in 1999 in six beagle dogs. Zone A is the biological seal — not a metaphor. Its integrity depends on mucosal thickness, keratinized tissue volume, and how gently the surgical approach treated the soft tissue.
Six beagle dogs, six fixtures per side, three months of healing after extraction, then another three after implant placement. Sacrifice, perfusion with fixative through the carotid arteries, EPON sections at 3 μm, PAS and toluidine blue staining. Moon, Berglundh, Abrahamsson, Linder, and Lindhe had one specific question: what is actually inside that band of connective tissue between the apical border of the junctional epithelium and the alveolar bone crest?
The answer appeared in the Journal of Clinical Periodontology in 1999. It has not become standard content in any implant course I have attended.
The geometry
The 200 μm analyzed — slightly more than the diameter of two hairs — were divided into two distinct units.
Zone A: the central 40 μm, immediately adjacent to the titanium surface. Absence of blood vessels, abundance of fibroblasts interspersed among thin collagen fibers. Histologically closer to periosteum than to gingiva.
Zone B: the lateral 160 μm, continuous with Zone A toward the external tissues. Fewer fibroblasts, thicker collagen fibers, blood vessels present. More similar to the gingival lamina propria.
Forty years ago we would have labeled all of that tissue “peri-implant connective tissue” and moved on. Moon et al.’s contribution was to dissect it — literally — into its functional components.
Why Zone A is avascular
The absence of vessels in Zone A is not a biological gap. It is a deliberate architecture. An avascular tissue is less penetrable, less prone to inflammation, and less responsive to bacterial toxins delivered hematogenously. The fibroblasts that populate it likely maintain active adhesion to the titanium surface — electron micrographs show them organized along the metal surface, not randomly distributed.
This is a gasket. Not a passive one — the fibroblasts maintain it actively. Where the titanium surface is clean and biocompatible and the connective tissue is intact, Zone A holds. Where there is chronic trauma, persistent plaque, or insufficient keratinized mucosa to physically accommodate both zones, it fails.
Zone A fibroblasts behave differently from gingival fibroblasts — and from the myofibroblasts that govern wound contraction in the early healing phase. Once the tissue matures around the implant, the seal zone settles into a stable, functionally specialized tissue that does not contract or remodel rapidly. That stability is the point.
The comparison with the natural tooth
Around a natural tooth the architecture is different: the periodontal ligament (PDL) anchors to cementum and bone through precisely oriented Sharpey’s fibers designed to withstand occlusal forces. That attachment is mechanically superior. The implant does not have it — we trade it for osseointegration, a direct bone-to-metal contact. The price of that trade is the soft-tissue seal: intrinsically less robust than what a tooth has.
This does not mean implants are fragile. It means Zone A cannot do the same job as cementum and the PDL. It can do its own job — sealing the interface between the oral environment and the peri-implant bone — if clinical conditions allow.
Those who study the differences between peri-implantitis and periodontitis at the microbiological level will find here one of the anatomical reasons why implants are structurally more vulnerable: the seal is thinner, less anchored, and lacks any cementum reserve.
Direct clinical implications
Keratinized tissue: Zone A and Zone B occupy physical space. Thin mucosa or fully alveolar mucosa does not leave the 200 μm needed to accommodate both zones functionally. The biological reason for requiring adequate keratinized tissue around implants is not cosmetic — it is geometric.
Mucosal thickness: a related but distinct concept. Thickness below 2 mm compromises the biology of both zones. Not aesthetically. Geometrically.
Surgical trauma: every incision and flap reflection disrupts the connective tissue in formation. Techniques that preserve the periosteum and overlying tissue — such as the osteo-mucosal expansion technique — create the conditions for Zone A to form on an already organized, undisrupted connective bed. What happens in the first minutes after a titanium surface contacts blood and tissue fluids sets the trajectory for everything that follows, including Zone A maturation.
Limitations
This is an animal study in beagle dogs. The measurements — 40 μm for Zone A, 160 μm for Zone B — are not transferable to human clinical practice as absolute values. The beagle’s microbiological profile, the fixture dimensions, the healing timelines: all are different.
What transfers is the principle: a two-zone functional organization exists, is reproducible, and has functional correlates. Subsequent studies in humans from the same Göteborg group and from others confirmed the presence of a connective zone adjacent to the implant that is functionally distinct from the surrounding mucosa. The numbers change; the geometry does not.
Questions
If I place the implant in a zone with sufficient keratinized tissue, does Zone A always form? Not automatically. Keratinized tissue creates the necessary conditions, not the sufficient ones. Implant surface, vertical positioning, mucosal thickness, occlusal load management — all influence the quality of the tissue that forms. Keratinized tissue is the precondition. Not the guarantee.
Can I assess Zone A clinically? No, not in vivo with current technology. It is visible on biopsy or at autopsy. Clinically, you monitor its favorable conditions indirectly: adequate mucosal thickness, absent BOP, no progressive pockets, stable crestal bone over time. When these indicators are stable, Zone A is probably doing its job.
Is a 1999 paper still relevant? It is relevant because no one has refuted it. Biology does not expire. The clinical implications — keratinized tissue requirements, soft-tissue respect during surgery, vertical implant positioning — derive from that histological principle. Changing implant brands does not change Zone A.
Are you biased on this topic? I practice techniques that preserve peri-implant soft tissue. So yes. But Zone A was described by Jan Lindhe, who has never operated in Frosinone.
Reference
Moon IS, Berglundh T, Abrahamsson I, Linder E, Lindhe J. The barrier between the keratinized mucosa and the dental implant. An experimental study in the dog. J Clin Periodontol. 1999;26(10):658-63. doi:10.1034/j.1600-051x.1999.261005.x. PMID: 10522777.
References
Looking for a specialist?
Implantologia a Frosinone →Impianti dentali, carico immediato e rigenerazione ossea
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stai valutando un impianto dentale?
Ho scritto una guida in 8 capitoli che spiega tutto quello che un paziente dovrebbe sapere prima di sedersi in poltrona. Niente marketing — solo fatti, casi studio e una checklist per fare le domande giuste.
Scarica la guidaStay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment