Non-Surgical Treatment of Peri-Implantitis with the TST Technique
At a glance — Severe peri-implantitis on a three-implant splinted bridge in a 95-year-old patient in good general health. Strictly non-surgical (flapless) treatment: TST decontamination — 10 seconds of HybenX plus air polishing with sodium bicarbonate — repeated every 6 months. Eight years of serial radiographs document progressive, stable bone fill of the vertical defects with maintenance of the crestal level. Clinical case by Dr. Marianna De Nale.
There is an almost automatic reflex when facing severe peri-implantitis: open, clean, regenerate. Surgical treatment often remains the reference choice. But not for everyone, and not always. This case tells the other story — the one without a scalpel — carried out with consistency for eight years.
The clinical picture
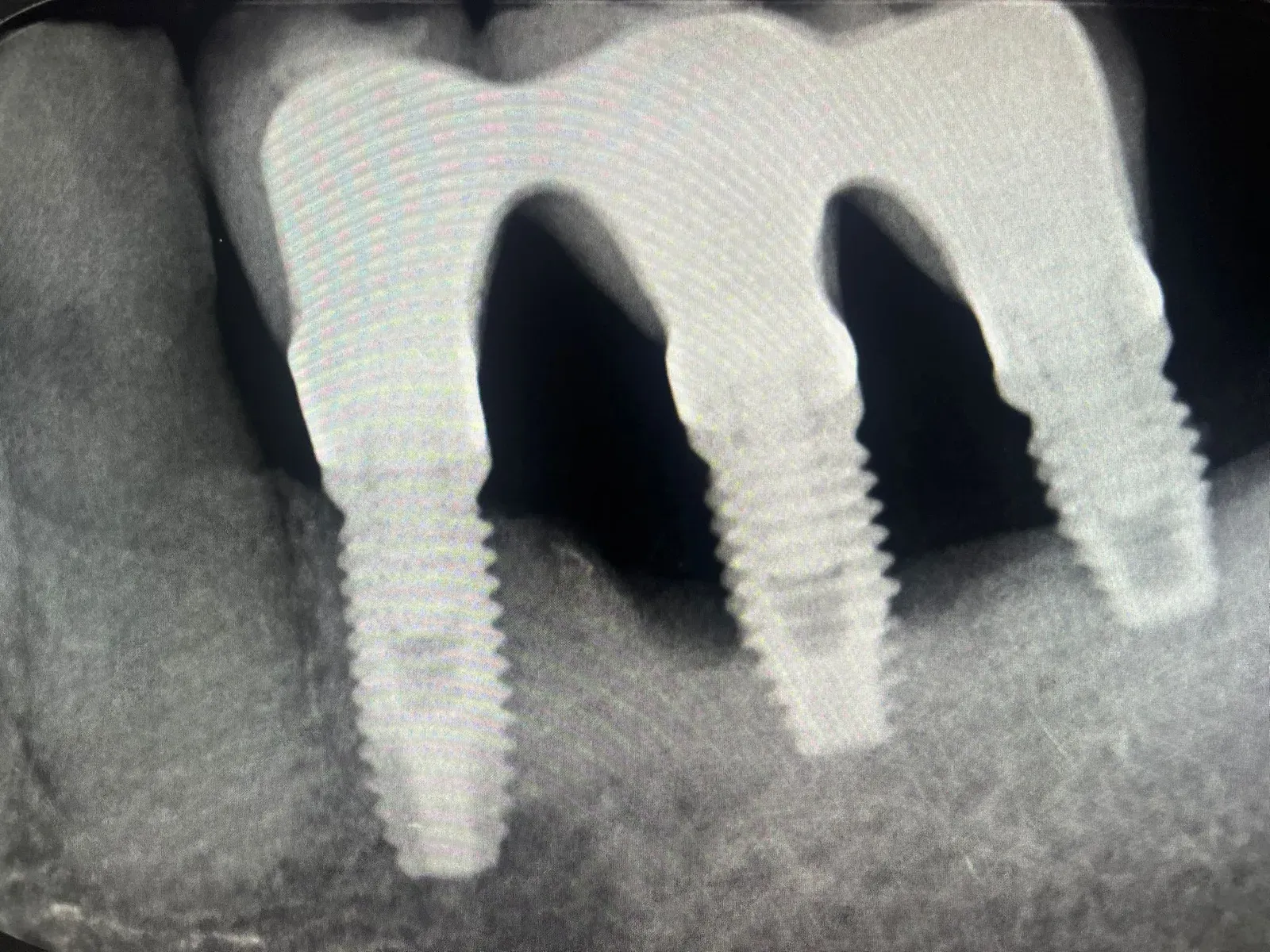
A 95-year-old patient in good general health. A bridge on three splinted implants in the posterior sector. Advanced peri-implantitis: vertical bone defects, exposed threads, radiographically documented bone loss.
The question here was not how to operate. It was whether to operate. At 95, every surgery — even the most contained — must be weighed: anaesthetic risk, tissue healing, the post-operative course, home management. The patient was well. The goal was to keep her that way.
A decision: no flap
The choice was to treat without opening. No incision, no sutures, no flap to manage post-operatively. Everything through the peri-implant sulcus.
The limitation of this approach is well known and should be stated up front: without exposing the defect, access to the contaminated surface is partial. It is a trade-off. You accept it when the risk-benefit ratio of surgery tips, as it does here, clearly toward caution.
The TST protocol, non-surgical version
The sequence is that of the Ten Second Technique, adapted to a closed field.
First step: HybenX gel applied for ten seconds to the implant surface reachable through the sulcus. Ten seconds, then a thorough rinse. HybenX acts through osmotic dehydration and denaturation of the biofilm, detaching it from the titanium surface without aggressive mechanical instrumentation.
Second step: air polishing with sodium bicarbonate, EMS Comfor+ 40-micron powder, for final decontamination. It removes the organic and mineral residues, completing the cleaning of the sulcus.

The in vitro validation of the TST was published in Scientific Reports by De Nale et al. [1]: SEM and EDX analysis showed effective biofilm removal with an intact implant surface. Here that protocol leaves the laboratory and the operating room and enters the chairside maintenance visit.
Eight years of follow-up, every six months
The real point is not the single session. It is the repetition.
TST decontamination was repeated every 6 months for 8 years (2018–2026). Each recall: reassessment, decontamination, radiographic check. Without this rhythm the result would not exist — peri-implantitis is an infection, and an infection is not “closed,” it is controlled.

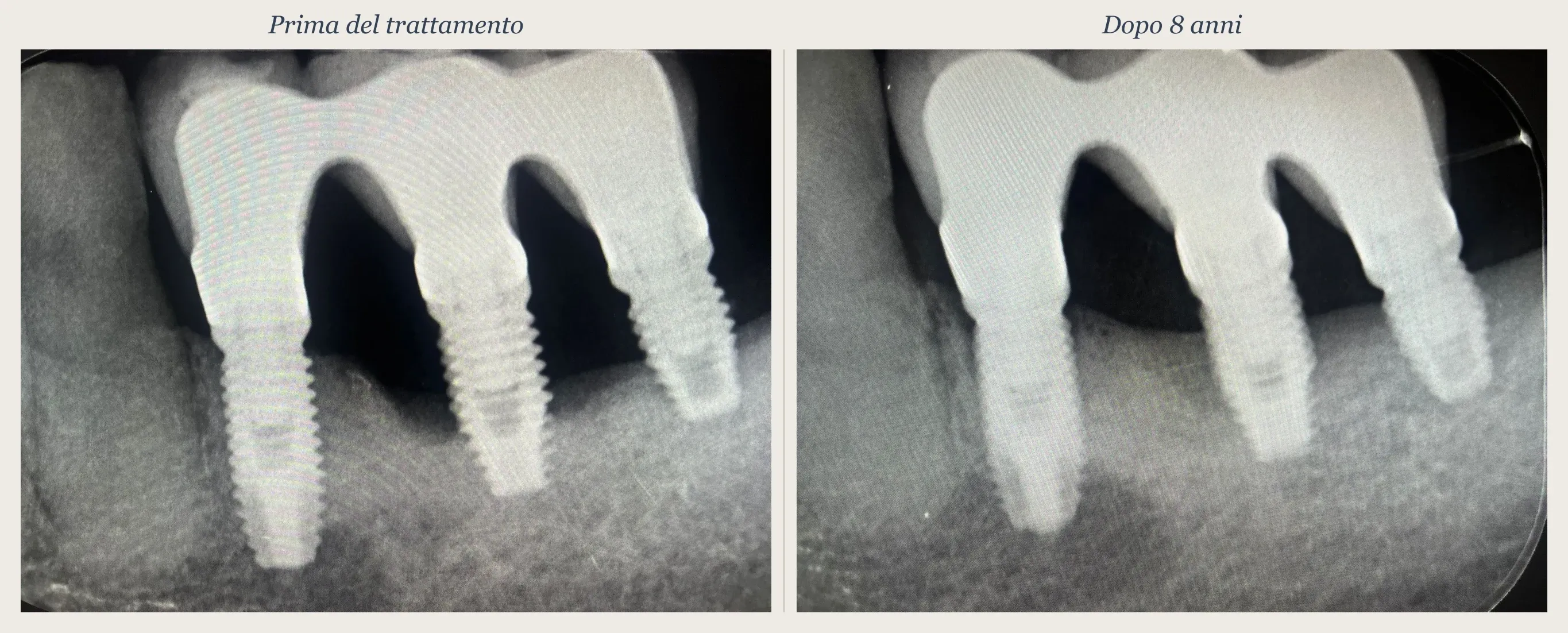
The serial radiographs tell a consistent story: the original vertical defects fill in progressively, the peri-implant bone regenerates, the crestal level at the end of treatment is fully recovered. No progression of bone loss. The bridge is in function.

The before/after comparison

What this case shows
That a minimally invasive approach, repeated with consistency and with the right tools, can achieve on an implant surface results that many would have entrusted to the scalpel. And in a patient for whom any surgery would have required serious consideration.
It must be said honestly what this case is not. It is not a study. It is not proof that non-surgical equals surgical. The literature on non-surgical air polishing in peri-implant disease is heterogeneous, and a recent systematic review with meta-analysis urges caution: the added clinical benefits are not consistent across studies [2]. The treatment of peri-implantitis remains a case-by-case decision in which decontamination, defect morphology and the maintenance programme all weigh together [3].
At 95 the right question is not “what is the best treatment in absolute terms,” but “what is the best treatment for this patient.” Sometimes the answer is not to open — and then not to give up for eight years.
Clinical case by Dr. Marianna De Nale — Private practice, Padua.
References
- De Nale M, Dalla Corte L, Bruschi E, Visentin F. An in vitro study exploring a new method for managing peri-implant disease using the ten second technique. Sci Rep. 2025;15(1):24870. DOI: 10.1038/s41598-025-08946-8
- Huang N, Li Y, Chen H, et al. The clinical efficacy of powder air-polishing in the non-surgical treatment of peri-implant diseases: a systematic review and meta-analysis. Jpn Dent Sci Rev. 2024;60:163-174. DOI: 10.1016/j.jdsr.2024.05.003
- Hong I, Koo KT, Oh SY, et al. Comprehensive treatment protocol for peri-implantitis: an up-to-date narrative review. J Periodontal Implant Sci. 2024;54(5):295-308. DOI: 10.5051/jpis.2303360168
FAQ
What does non-surgical TST treatment of peri-implantitis involve?
When can surgery be avoided in peri-implantitis?
How often does the treatment need to be repeated?
Can non-surgical decontamination really regenerate bone?
What is the difference between surgical and non-surgical TST?
References
Looking for a specialist?
Implantologia a Frosinone →Impianti dentali, carico immediato e rigenerazione ossea
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stai valutando un impianto dentale?
Ho scritto una guida in 8 capitoli che spiega tutto quello che un paziente dovrebbe sapere prima di sedersi in poltrona. Niente marketing — solo fatti, casi studio e una checklist per fare le domande giuste.
Scarica la guidaStay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment