"Bind me!" Blood and Titanium: love is born in five minutes.
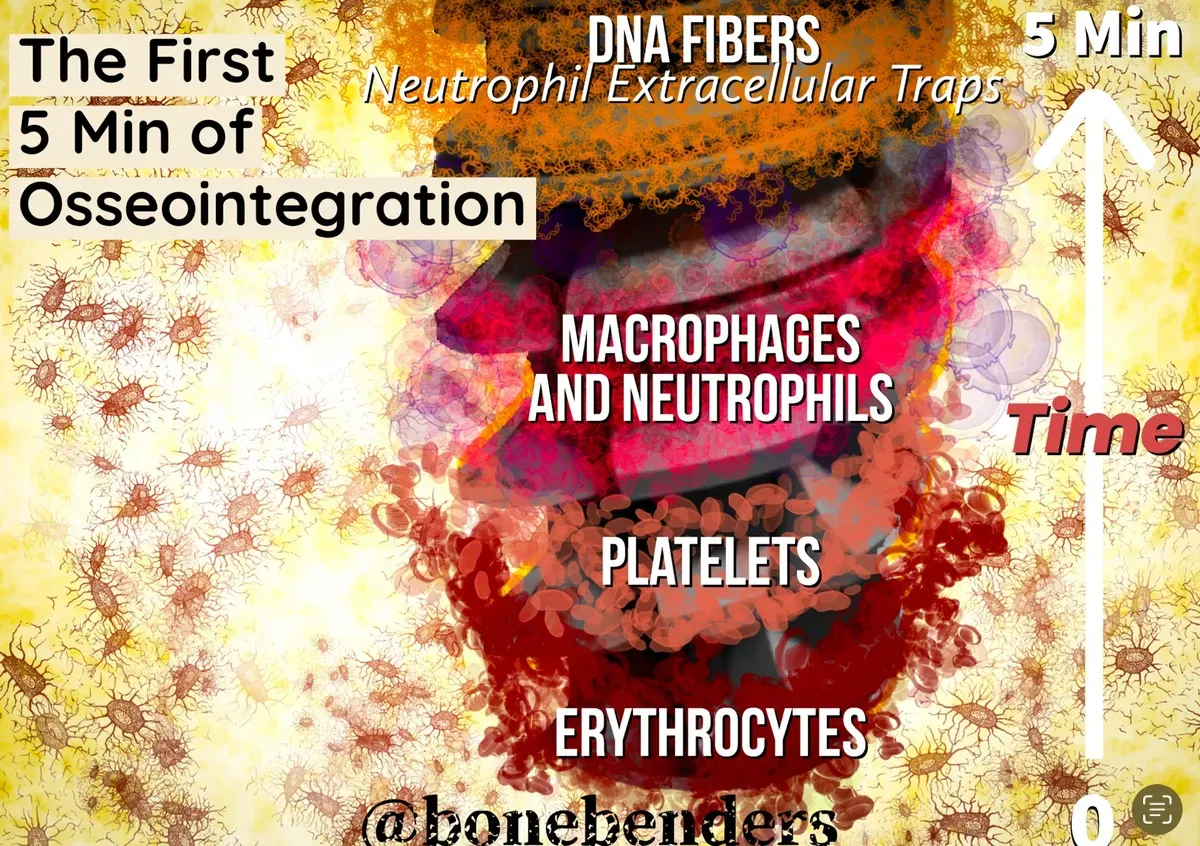
In brief — In the first five minutes after implant insertion, blood deposits a complex layer of proteins on the titanium surface in a precise sequence (the Vroman effect). Surface roughness determines the abundance and type of adsorbed proteins, directly influencing the success of osseointegration. Rough surfaces attract greater quantities of fibronectin, complement factors and inflammatory mediators essential to the healing process.
Implants are like people: the first contact is the most important. The first impression can be favourable, or not.
The bone integration process is still not fully understood, but it certainly involves a sequence of protein adsorption, cell migration, proliferation and bone deposition.
The Vroman effect
According to the Vroman effect, smaller proteins at higher concentrations tend to adsorb to the surface first, and are later replaced by larger proteins with higher binding affinity. So the longer the incubation time, the more the protein composition (the proteome) on a given surface changes.
In a remarkable recent study on orthopaedic titanium implants (Jäger et al., 2022), researchers showed that within the first five minutes a process unfolds that is as crucial as it is fascinating.
Proteins and mechanical anchors
A close analysis of the implant surface proteome at two telling moments — 2 and 5 minutes after insertion — reveals an abundance of proteins on the rougher implant surfaces.
For osseointegration to begin, then, it is crucial that proteins find mechanical anchoring points. The micro- and macro-structure of the implant surface plays a fundamental, imperative role throughout bone integration, far outweighing the importance of time alone.

It follows that implants lacking significant nano-, micro- and macro-geometry (machined surfaces) dramatically hinder this fundamental integration process.
Even if such surfaces may look attractive and promise certain advantages (limited to cleansability in case of peri-implantitis), it is absolutely crucial to weigh their potential risks and drawbacks.
Ignoring these factors can lead to unwanted and unpredictable consequences, making it imperative to consider both sides of the question carefully.
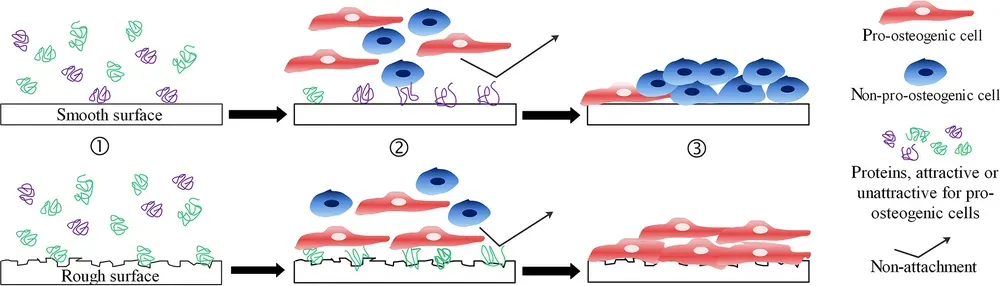
This is not just my conviction. A review by Kondo, Yamada and Egusa (Journal of Prosthodontic Research, 2024) brings exactly this into focus: surface microroughness and hydrophilicity do not merely recruit proteins. They re-educate the innate immune response. They dampen neutrophil inflammation, push macrophages toward an anti-inflammatory profile and, in doing so, govern both contact osteogenesis and distance osteogenesis — the kind that starts from the bone edges, away from the implant. It is the cellular proof of what I was saying: a smooth surface starts at a disadvantage.
[The figure below, from Stich et al., 2021 - CC Attribution 4.0 International licence - illustrates, cartoon-style, the difference between smooth and rough surfaces]
Bone extracellular matrix (ECM) proteins and their distribution within the implant surface proteome
How does the ECM evolve in the first five minutes?
The ECM is a fundamental component of tissues and organs, providing the structural support essential for bone integration.
Collagen makes up a full 90% of the organic ECM of bone, and its biosynthesis and biochemistry are decisive for this osseointegration.
Among the many bone ECM proteins, type I collagen — magnificently organised into fibrils with triple polypeptide helices — is the most abundant and the most fascinating.
Collagen fibrils interweave in an embrace with one another and with other proteins, assembling higher-order bundles and fibres that begin to lay out the geometry of the new bone structure. Several types of collagen bind firmly to the implant surface (provided it has the right micro- and macro-geometry).
The lightning-fast rise of type III collagen on the rough surface within five minutes
Again according to Jäger et al., 2022, the abundance of type I collagen is similar on rough and smooth surfaces at two minutes after exposure, but the real, decisive difference appears in the next phase. At 5 minutes the amount of type III collagen explodes on the rough surface, while it is far less represented on the smooth one.
Among the non-collagenous proteins, the low-molecular-weight leucine-rich proteoglycans are the most abundant in this early phase of healing bone ECM formation.
Glycoproteins such as thrombospondin, fibronectin and vitronectin are also part of the implant proteome.
Osteoblasts produce thrombospondins at various stages of bone maturation and development. Fibronectin and vitronectin come from plasma and interact with other ECM proteins, and are fundamental to the assembly of the collagen matrix itself.
Fibronectin, certain complement factors and inflammatory mediators rise sharply on the rough surface
On the rough surface, the fibronectin produced in the early phases of bone formation is upregulated compared with the smooth surface. The rough surface also stimulates the production of several complement factors, of certain inflammatory mediators (such as MMP9), and of the S100A9 protein, known to drive neutrophil chemotaxis and adhesion, which in turn is essential for osseointegration.
Haemostasis and inflammation
Did you know inflammation and haemostasis are two interconnected processes?
Inflammation triggers the activation of haemostasis, which plays a crucial role on the surface of a freshly inserted implant.
Haemostasis, the complement cascade and neutrophil degranulation activate the proteins that adhere to the implant surface.
How concrete this embrace between blood and titanium really is, two recent papers make clear. Lackington and colleagues (Advanced Healthcare Materials, 2024) texturised a titanium-zirconium alloy with a femtosecond laser and made it hydrophilic down to a 10° contact angle: in contact with whole human blood, this surface builds a fibrin network comparable to that of sandblasted and acid-etched surfaces, and at twenty-eight days it mineralises two and a half times more. Wettability, in other words, is no laboratory detail — it is what decides whether the first clot spreads out or retreats. On the other side, Ulusoy and colleagues (Clinical Implant Dentistry and Related Research, 2024) measured that a contaminated surface halves the adhesion of the fibrin clot to titanium. Surface cleanliness, then, is not a matter of form: it is the precondition for that first clot to take hold at all.
So it is essential to keep a balance at the bone-implant interface to avoid complications in the early phase of integration. In the early phases (and over time), even slight but persistent changes in the surrounding environment can significantly affect implant performance.
What happens, for instance, when microbial, inflammatory, immunological, medical, pharmacological and metabolic factors alter the equilibrium around the implant?
This perturbation can cause inflammation to re-emerge, foreign-body giant cells to form outside the “physiological” process, and osteoclastogenesis to be activated — all of which can lead to bone loss around the implant (known as peri-implant disease).
Which proteins potentially involve haemostasis and neutrophil activity in the first five minutes of osseointegration?
Haemostasis is a natural reaction (to prevent excessive blood loss and preserve volume for the rest of the body) in response to damage to blood vessels in the periosteum, bone and surrounding soft tissues during surgery.
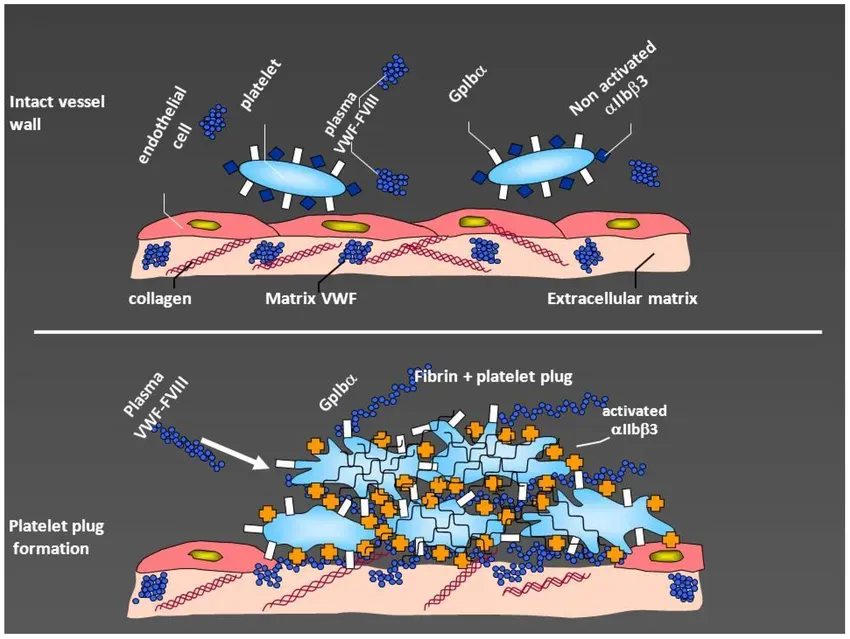
Platelets are the first to respond, through adhesion, aggregation and degranulation. In vivo, the disruption of the endothelial layer and the exposure of the underlying subendothelial matrix lead to platelet activation through interactions with collagen, fibronectin, von Willebrand factor and various platelet glycoprotein receptors.
Platelets not only play a vital role in haemostasis, they also have the power to activate the immune system. They achieve this through their receptors and granules, which contain a multitude of biologically active products.
P-selectin on activated platelets binds a specific receptor on the neutrophil surface, which switches on the immune response. Moreover, the CD40 ligand secreted by platelets regulates integrin expression on neutrophils, which is crucial to these mechanisms. The secretion of serotonin and platelet factor 4 leads to neutrophil recruitment and adhesion.
It is clear from the findings above that platelets are fundamental to a healthy immune system and play a significant role in the body’s defence mechanisms — among them wound healing and osseointegration.
The role of white blood cells in osseointegration
Plasma leucocyte concentration is higher than normal in all patients after surgery.
Neutrophils, basophils and eosinophils, which belong to the polymorphonuclear leucocyte group, make up 40-65% of the white blood cell population, and their elevated levels are a hallmark of acute inflammation.
Right after tissue injury (osteotomy, in our case), these cells exert antimicrobial activity through degranulation, enzyme release and the phagocytosis of foreign substances and debris.
Neutrophil extracellular traps (NETs) in the first five minutes
The body’s ability to integrate an implant into the surrounding tissue is truly remarkable.
A crucial step in this process involves the creation of the so-called neutrophil extracellular traps, which play a fundamental role in forming fibrous DNA-based networks.
Neutrophils release toxic substances such as elastase, myeloperoxidase, cathepsins and defensins, and these cause cellular damage that further facilitates this process. These proteins are present in the implant surface proteome.
The rapid enrichment of myeloperoxidase and cathepsin G on the rough surface after 2 and 5 minutes is particularly noteworthy. These DNA networks are essential to set in motion the processes that lead to successful osseointegration.
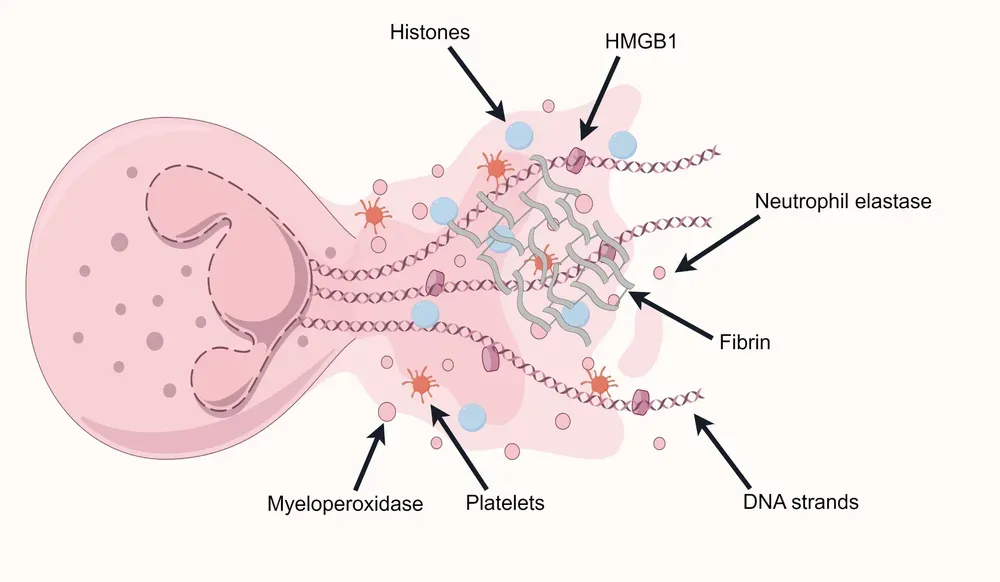
[Figure from Liu et al., 2025 - CC Attribution 4.0 International licence]
Myeloperoxidase catalyses the formation of reactive oxygen species, while cathepsin G stimulates the production of cytokines and chemokines responsible for activating and mobilising immune cells.
This process highlights the extraordinary resilience and adaptability of the human body.
Neutrophil recruitment through DAMPs and the complement system
Surgery-induced tissue damage causes the release of damage-associated molecular patterns (DAMPs) by necrotic cells into the extracellular space, which activate neutrophils and trigger a sterile inflammatory response.
These DAMPs include extracellular ATP, formylated peptides, mitochondrial DNA, nucleic acids, heat shock protein, S100 protein, high-mobility group box 1 protein and altered extracellular matrix components such as hyaluronan.
It is worth noting that these same proteins have also been found in the implant proteome.
This information is fundamental to advancing our understanding of the healing process and to developing effective treatments. The power of these molecules to activate neutrophils and trigger inflammation is undeniable, and harnessing it could have significant implications for medicine and health.
Complement
Insertion of the titanium implant activates the complement system. The complement system, in turn, is another pathway that recruits neutrophils to the implant site, and this occurs through the classical pathway but is further amplified via the alternative pathway.
Several complement factors — including complement factor B (CFB), C3, C4 and C5 — are present in the proteome on the implant surface. Studies show that these factors are significantly enriched on both rough and smooth implant surfaces after a two-minute exposure time.
The proteins produced by osteocytes, osteoclasts and osteoblasts
Bone cells, moreover, can produce complement factors and are themselves targets of complement. Osteoblasts can produce C3 and C5, while osteoclasts can release activated C5a.
The anaphylatoxins C3a and C5a are chemotactic for neutrophils and for osteoblasts and their precursors, the mesenchymal stem cells. In osteoblasts, they stimulate the release of inflammatory cytokines, including IL-6 and IL-8. In addition, C5a can stimulate the secretion of osteoclastogenic factors.
Therefore, the activation of the complement system could directly influence bone healing too, by interacting with bone cells. Enhanced osteoclastogenesis could increase bone resorption, while the recruitment of osteoblasts and their precursor cells promotes bone formation.
In recent years this interplay between immunity and bone has earned a name: osteoimmunology. A review by Yun and colleagues (International Journal of Molecular Sciences, 2025) goes one step further, and proposes that “osseointegration” is almost a reductive term: speaking of osteoimmunologic integration describes better what actually happens. The bone that forms around the implant is also a form of the organism’s defence against a foreign body, orchestrated by regulatory T cells and macrophages. I like this idea, because it gives bone back its true nature — not inert cement, but living tissue that remodels continuously between osteoclasts, osteoblasts and osteocytes. Understanding this dialogue is the first step toward learning how to steer it.
References
- Jäger M, Jennissen HP, Haversath M, et al. Capacity of the Surface Proteome of Titanium Implants to Modulate the Early Immune Response. J Funct Biomater. 2022;13(2):44. doi:10.3390/jfb13020044 · PMID: 35466226
- Stich T, Alagboso F, Křenek T, et al. Implant-bone-interface: Reviewing the impact of titanium surface modifications on osteogenic processes in vitro and in vivo. Bioeng Transl Med. 2021;7(1):e10239. doi:10.1002/btm2.10239 · PMID: 35079626
- Kondo T, Yamada M, Egusa H. Innate immune regulation in dental implant osseointegration. J Prosthodont Res. 2024;68(4):511-521. doi:10.2186/jpr.JPR_D_23_00198 · PMID: 38346728
- Lackington WA, Bellon B, Guimond S, et al. Bio-Inspired Micro- and Nano-Scale Surface Features Produced by Femtosecond Laser-Texturing Enhance TiZr-Implant Osseointegration. Adv Healthc Mater. 2024;13(23):e2400810. doi:10.1002/adhm.202400810 · PMID: 38857489
- Yun JI, Yun SI, Kim JH, Kim DG, Lee DW. Mediation of Osseointegration, Osteoimmunology, and Osteoimmunologic Integration by Tregs and Macrophages: A Narrative Review. Int J Mol Sci. 2025;26(11):5421. doi:10.3390/ijms26115421 · PMID: 40508228
- Ulusoy HÖ, Ercan E, Özatik O, Tunalı M. Fibrin clot adherence on cleaned and decontaminated titanium abutment surfaces: An in vitro study. Clin Implant Dent Relat Res. 2024;26(6):1190-1199. doi:10.1111/cid.13366 · PMID: 39210678
FAQ
Why are the first five minutes so crucial in osseointegration?
Why does implant surface roughness matter so much?
How does the Vroman effect work in clinical practice?
What is the role of fibronectin and glycoproteins in osseointegration?
References
- https://doi.org/10.1002/btm2.10239
- https://doi.org/10.3390/jfb13020044
- https://doi.org/10.2186/jpr.JPR_D_23_00198
- https://doi.org/10.1002/adhm.202400810
- https://doi.org/10.3390/ijms26115421
- https://doi.org/10.1111/cid.13366
- https://doi.org/10.1186/s40364-025-00731-z
- https://pubmed.ncbi.nlm.nih.gov/35466226/
- https://pubmed.ncbi.nlm.nih.gov/35079626/
- https://pubmed.ncbi.nlm.nih.gov/38346728/
- https://pubmed.ncbi.nlm.nih.gov/38857489/
- https://pubmed.ncbi.nlm.nih.gov/40508228/
- https://pubmed.ncbi.nlm.nih.gov/39210678/
Go deeper
Espansione crestale (split crest) →Allargare la cresta senza trapianto — tecnica ERE e bonebending
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stai valutando un impianto dentale?
Ho scritto una guida in 8 capitoli che spiega tutto quello che un paziente dovrebbe sapere prima di sedersi in poltrona. Niente marketing — solo fatti, casi studio e una checklist per fare le domande giuste.
Scarica la guidaStay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment