Ode to the Hidden Buttress of the Upper Jaw
Summary (EN) — In the upper jaw there is a bony arch that does not fit among the classic vertical and horizontal buttresses of the skull. It is hidden inside the splanchnocranium and runs along the curve that joins the nasopalatine recess, the base of the canine buttress, and the anterior nasal spine. I call it the «supramaxillary arch» — a term and concept I devised myself, published on Zenodo, not a textbook entry. Knowing it and recognising it matters.
Our natural tendency is to think on a plane. We are used to drawing up treatment plans — at least the less complex ones — on two-dimensional radiographs. The panoramic is a classic.
Two dimensions are a limit. The world is three-dimensional. And the fourth dimension, time, is just as fundamentally important. That is true in our field too.
With the advent and spread of CBCT, this way of thinking has changed and is still changing. But a strange legacy of entrenched habits remains. They are hard to uproot. I see it often in planning maxillary sinus crestal lifts, for example. Many colleagues struggle to picture local anatomy in three dimensions. And so many interesting therapeutic opportunities are missed.
The buttress they skip in courses: the Supramaxillary Arch
The term «supramaxillary arch» and the idea of treating it as a single arch linking the three segments below are my own conceptual framework — published as a technical note on Zenodo — a clinical taxonomy I use to navigate CBCT. The individual anatomical landmarks exist in the literature; the arch as an integrated concept does not. I state this upfront so we do not confuse official nomenclature with an operative model.
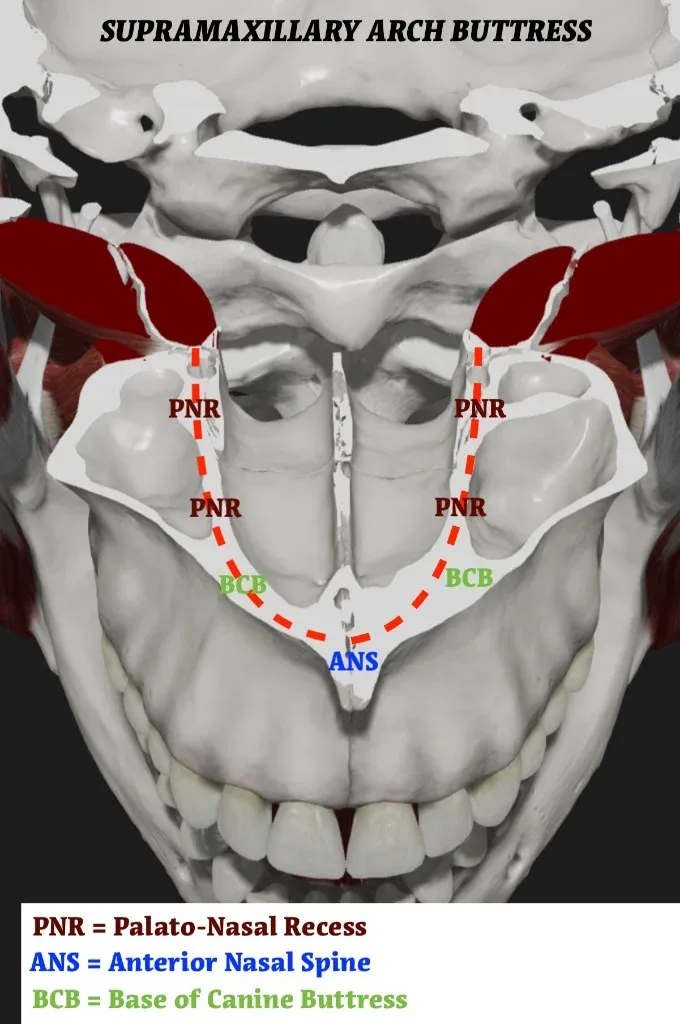
It is a fundamental structure for the lateral resistance of the splanchnocranium. It is formed by the union of the following bony segments:
- The nasopalatine recess (PNR, palatonasal recess): the angle between the medial wall of the maxillary sinus floor and the lateral wall of the nasal cavity that separates it from the rest of the upper aerodigestive tract.
- The base of the canine buttress: the vestibular bony eminence supporting the canine, posterior to the canine fossa and anterior to the nasal margin.
- The anterior nasal spine: together with the maxillary frontal processes that form the bony base of the piriform aperture, cranial to the nasoalveolar clivus.
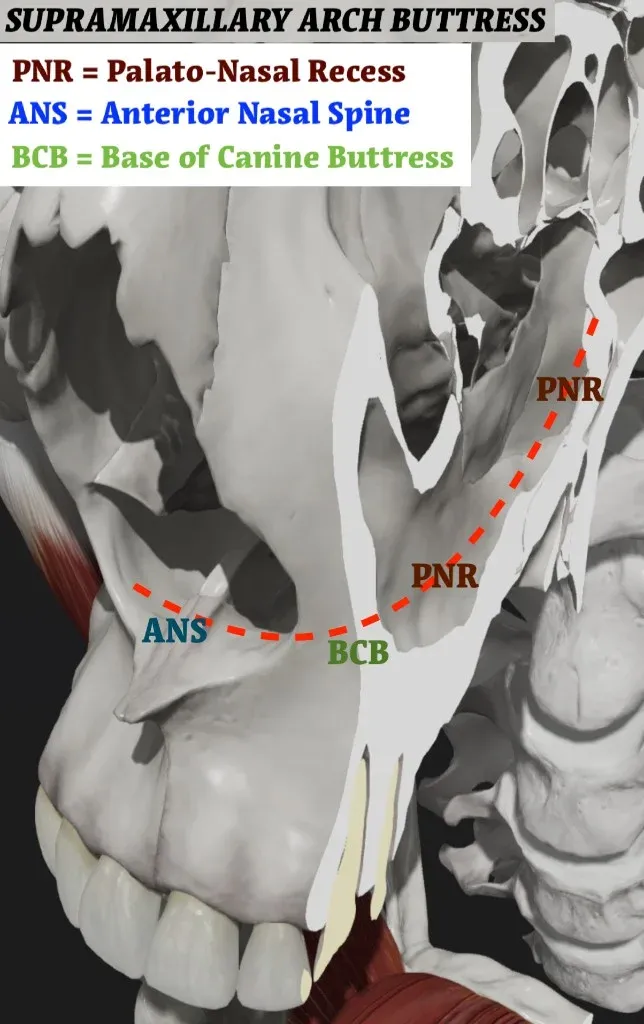
On a lateral section, the arch reads as a continuous curve linking the three vertices — PNR, base of the canine buttress (BCB), and anterior nasal spine (ANS):
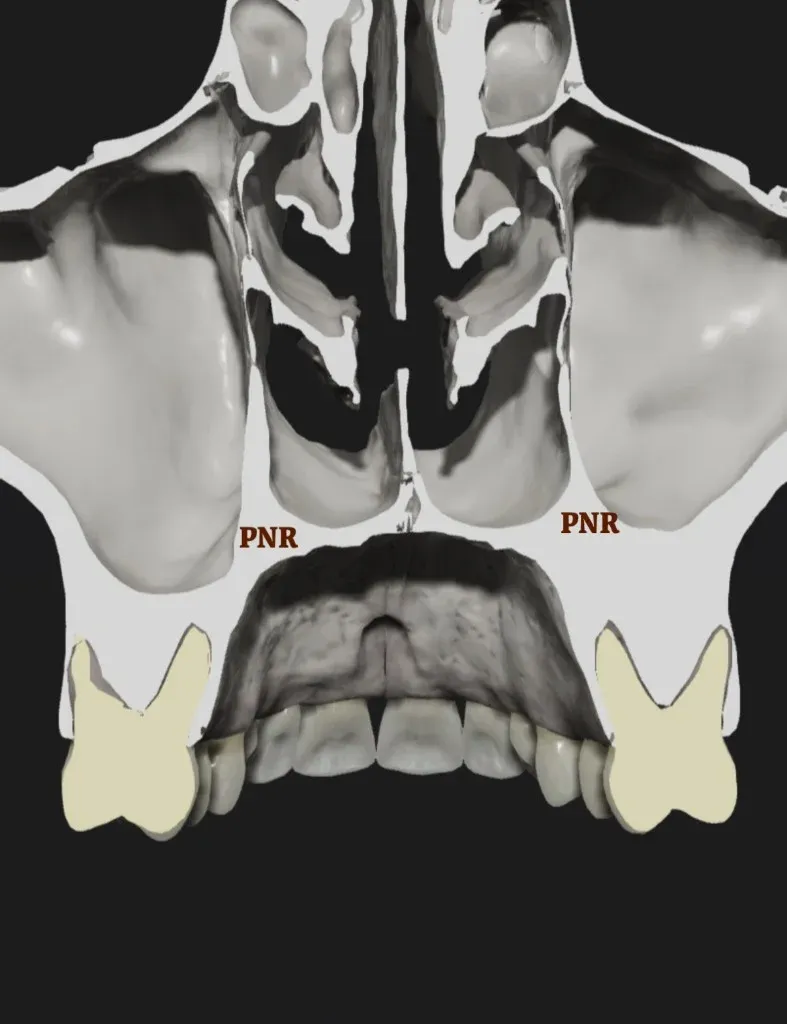
First segment of the arch: the nasopalatine recess
On a sagittal section, the PNR sits at the angle between the medial floor of the maxillary sinus and the lateral wall of the nasal cavity — exactly where the Schneiderian membrane meets bony resistance during lateral-window lift.
Until Chan et al. measured the PNR angle systematically in 2013, the term did not appear in major sinus lift protocols. Nobody looked for it. Now we know it is there, that it forms a measurable angle on CBCT, and that the geometry of this angle matters when planning the intervention.
On 274 edentulous sites analysed with CBCT, the PNR sits on average 14.2 mm from the crest at the second premolar, 12.5 mm at the second molar. Mean angulation runs from 109.8° at the premolar to 144.9° at the molar. Translation: at the premolar the recess is closer to the crest and more acute.
For anyone performing maxillary sinus lift via lateral window, the consequence is concrete. An acute recess increases tension and is generally accompanied by a large sinus, which will heal more slowly because both vascularisation and the source of progenitor cells are reduced.
Second segment of the arch: the base of the canine buttress
The canine is not «just» the longest tooth in the arch. It sits inside one of the most important buttresses of the skull.
Schuh et al., studying human maxillary ontogeny with surface histology and geometric morphometrics on 47 skulls aged 0 to 12 years, showed that the canine fossa arises from the interaction of localised bone resorption and growth in the surrounding field. It is a fascinating mechanism, common to the whole splanchnocranium — the same continuous remodelling that governs implant survival. The canine buttress absorbs and redistributes masticatory forces toward the base of the upper jaw.
Zhang, Skrypczak, and Weltman measured anterior alveolar dimensions on CBCT for immediate implant planning. The canine region shows the greatest bucco-lingual width at the crest among the three anterior teeth and the lowest risk of fenestrating the vestibular cortex. The lateral incisor? The most dangerous: thinnest ridge, most coronally positioned buccal undercut, highest probability of perforation in immediate implant placement.
Todorovic et al., with micro-CT on 72 skulls, closed the loop with numbers that make you think: the anterior buccal cortex rarely exceeds 0.5 mm. Buccal fenestrations in up to 33.8% of cases. On the palatal side, canine thickness reaches 5.43 mm at 9 mm from the crest. The canine buttress is a key biomechanical strong point — primary stability runs through it when the vestibular crest is tissue paper. Anchorage can shift to the palatal side, and it runs through the buttress base.
Third segment of the arch: the anterior nasal spine and adjacent bony structures
The piriform aperture frames the entrance to the nasal cavity. Its inferior margin — the anterior nasal spine and the maxillary frontal processes — marks the cranial boundary of the anterior implantable sector.
Two problems converge here that two-dimensional planning undervalues. First: proximity of the nasopalatine canal. Second: morphological variability of the anterior nasal spine, which conditions labial bone thickness and implant axis inclination.
Calin et al., in a 2025 multicenter study of 150 CBCT scans, analysed incisive canal characteristics for cortical anchorage potential. Mean length 10.27 mm, mean width 3.55 mm — but more importantly, significant correlations between canal diameter at the palatal base and distance to the labial cortex (r = 0.67). Wider canals mean more cortical bone available around them. In maxillae with little bone, that cortex can become the only anchor.
Do not confuse the canal with the recess. The canal is the anterior midline conduit. The recess is the posteromedial angle of the sinus. Both belong to the same arch, but they answer to different surgical logics.
Anatomical variability
The arch is not the same in everyone. The big-nose maxillary variant shifts the naso-sinusal boundary and redraws the PNR. Tooth loss accelerates bone resorption of the nasoalveolar clivus. But in essence, the approach does not change.
Look where others scroll past
The next CBCT you open for an upper jaw, try this. Sagittal at the premolar: measure the PNR angle. Coronal at the canine: mark palatal thickness at 3, 6, 9 mm. Axial at the piriform aperture: trace the nasopalatine canal and check the base of the piriform opening.
FAQ
What is the «supramaxillary arch» and why does it matter for implants?
Is the nasopalatine recess the same as the nasopalatine canal?
Why is the canine region preferable to the incisors for anchorage?
Does an acutely angled PNR always complicate maxillary sinus lift?
Can an implant be anchored in the nasopalatine canal?
Why should I trust you on an anatomical ode rather than the textbook on my shelf?
References
Looking for a specialist?
Implantologia a Frosinone →Impianti dentali, carico immediato e rigenerazione ossea
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stai valutando un impianto dentale?
Ho scritto una guida in 8 capitoli che spiega tutto quello che un paziente dovrebbe sapere prima di sedersi in poltrona. Niente marketing — solo fatti, casi studio e una checklist per fare le domande giuste.
Scarica la guidaStay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment