They Lied to You About Primary Stability
In brief — Primary stability is friction: it always requires bone compression. The dogma of the “passive” implant is false. The real skill is choosing where and how much to compress based on the specific anatomy, not avoiding compression altogether.
Sintesi (IT) — La stabilità primaria è attrito: esige sempre compressione ossea. Il dogma dell’impianto “passivo” è falso. La vera arte è scegliere dove e quanto comprimere in base all’anatomia, non evitare la compressione.
And you don’t even know it
Let me ask you an uncomfortable question: how many times have you placed a dental implant chasing “that feeling” of stability, convinced you were doing the right thing? And how many times did a doubt creep in — that the very force you were applying might cause “compression necrosis” of the bone?
The truth nobody has the courage to tell you: passive implants do not exist. For an implant to be stable, it must compress the bone. Full stop.
It’s a fairy tale the industry and many opinion leaders have told for years, and one we swallowed without asking questions.
It belongs to that set of granite-solid certainties on which we base our daily clinical choices in implant dentistry — certainties that often rest on foundations of sand. The ideas of yesterday’s opinion leaders matter a great deal, but they are not, necessarily, scientific truth.
Sounds impossible? Keep reading, because I’m about to take apart, piece by piece, some of the most deeply rooted convictions of modern implantology. And I warn you: what you discover might make you reconsider everything you thought you knew about the primary stability of dental implants.
From scientific research to clinical practice
I came across a beautiful article by Nikos Mattheos that gave me further confirmation on themes I hold dear.
I’ve reworked it to share with you concepts that should change the way we think about dental implants.
Nikos Mattheos’s full blog is here: https://mattheos.net/
Bone compression in dental implants: necessary, not optional
Let’s be blunt: every time a dental implant is clinically stable after placement, it is compressing bone somewhere.
There’s no escape. It’s basic physics — the kind they taught us in high school and we forgot the moment we left the classroom. Static friction, the thing that gives us so-called “primary stability,” cannot exist without a force acting between two adjacent surfaces. In our case, that force is bone compression.
So when someone tells you their implant doesn’t compress bone because it has few threads, they’re simply shifting the compression onto the body of the implant. They are not eliminating it, because… they can’t!
If they really managed to eliminate compression, their implant would spin in the osteotomy like a stripped screw. We need to stop accepting this kind of nonsense.
And yet for years we classified dental implants as “aggressive” or “passive” based mainly on the look of their threads. It’s like judging a book by its cover.
A conceptual error so crude it’s almost endearing — if it weren’t for the fact that on this error we built clinical protocols and made decisions that affected our patients. If you still believe smooth implants are better, it’s time to revisit that conviction.
Histological studies on osseointegration: the truth you’ve always read wrong
Now for the centerpiece. Remember those historic studies from the Göteborg team? The ones with the gorgeous histological images showing bone resorption at the threads on day four?
Of course you remember them. They’re the studies that terrified entire generations of implantologists into fleeing from implants with pronounced threads.
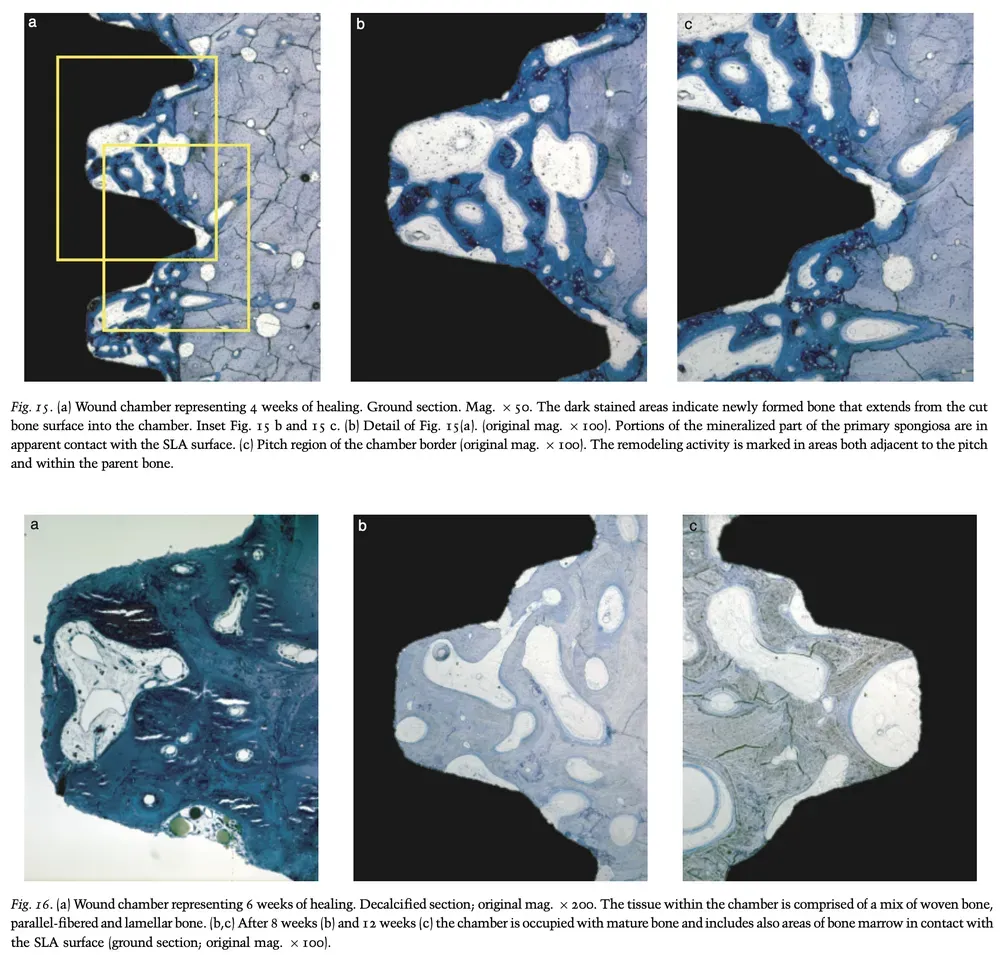
But here’s what nobody ever really explained to you: while everyone obsessed over resorption at the threads, something extraordinary was happening in the non-contact chambers.
New bone forming on the implant surface where before there had been only clot. This phenomenon, which today we call contact osteogenesis, depends heavily on the interaction between blood and the titanium surface in the first minutes after implant placement.
The full message was clear: yes, compression causes localized resorption, but at the same time, in the non-contact spaces, new bone forms.
It’s a dynamic, complex process that cannot be reduced to the simplistic mantra compression = bad. And yet that is exactly what happened.
We took half the truth and built a dogma on top of it. And we forgot that the competition between osteoblasts and myofibroblasts in the early phase decides whether we get osseointegration or fibrointegration.
The primary-vs-secondary stability graph: speculation or science?
And now, the coup de grâce.
You know that iconic graph showing primary stability progressively decreasing while secondary stability rises, with that famous “stability dip” in the middle? The one we all used to explain why we shouldn’t load implants immediately?
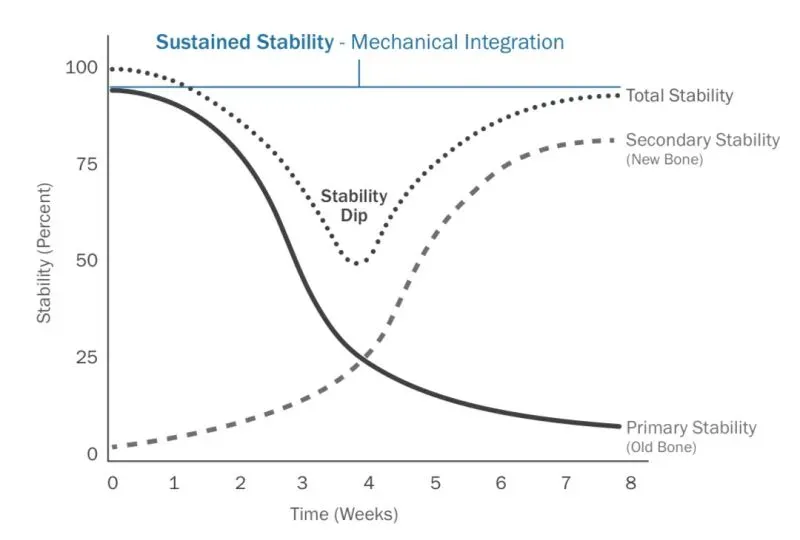
That curve is pure speculation. It has never been clinically demonstrated. Never.
It was extrapolated from interpretations of histological bone-to-implant contact studies, but the logical leap from “BIC percentage” to “actual clinical stability” was never validated.
It might match reality. It might be false. It might be far more complex than that. The reality is, we don’t know. What we do know is that metabolic factors such as vitamin D3 significantly influence osseointegration — and that appears in no traditional graph.
And yet that curve became a pillar of implant teaching worldwide.
The most recent literature pulls more ground out from under it. A 2026 systematic review with meta-analysis by Tisci and colleagues at the University of Foggia, published in Clinical Implant Dentistry and Related Research, pooled 48 studies and found that ISQ — the number you read on your Penguin or Osstell and trust your decisions to — correlates only moderately with insertion torque (r = 0.44), with very high heterogeneity. Worse: ISQ values at placement do not predict marginal bone loss or implant survival. Translation: the little number many use as an oracle is a complementary indicator of friction, not a crystal ball on the fate of the implant.
Friction stability: the concept that changes everything in implantology
Let’s call it by its real name: friction stability. Not “primary,” not “initial,” not “mechanical.” Friction.
Because that’s exactly what it is. And friction depends on how hard you press two surfaces together. In our case, on how much force the implant surface exerts on the bone surface.
This change in terminology isn’t academic pedantry. It’s conceptual clarity that leads to better clinical decisions in implant dentistry.
Because if you understand that you’re looking for friction, you also understand that you have to compress bone somewhere. And then you stop hunting for the magical implant that doesn’t compress, and you start reasoning about where and how much you want to compress based on the specific case.
And here the other fetish collapses too: the threshold numbers. How many people taught you that you need at least 35 N·cm of torque, or an ISQ above 60, otherwise the implant is “unstable”? A 2025 systematic review with meta-analysis by Razaghi and colleagues, published in the International Journal of Prosthodontics, analyzed 79 studies and found no evidence that a torque ≥ 35 N·cm or an ISQ ≥ 60 guarantees higher survival than lower values — at least for non-immediately loaded implants: implants placed with ISQ < 60 survived in 97.7% of cases. Along the same line, Darriba and colleagues, back in 2023 in the Journal of Clinical Periodontology, showed that even in immediate loading a low torque (≤ 35 N·cm) gave 96% survival, statistically identical to the 92% of high torque. The moral isn’t “push hard” or “push gently”: it’s that the number alone doesn’t tell the story. The problem is never the little figure on the ratchet — it’s what you’re doing to the bone.
Threads compress at precise points. The wedge effect distributes compression over wider surfaces. And which of the two makes sense is decided by the bone in front of you, not by the company’s brochure.
The data say so too. A 2023 systematic review with meta-analysis by Putra and colleagues, published in Clinical Oral Implants Research, gathered 26 studies and over 3,000 implants and quantified what every surgeon feels in their fingers: bone density and cortical thickness correlate with primary stability (ISQ r = 0.60; torque r = 0.52). Where the cortex is thick, friction comes on its own; where the bone is soft, you have to go looking for it. That’s why reading the anatomy well beforehand — the Wang alveolar bone classification exists for exactly this — matters more than any implant macrogeometry choice made at the desk.
There’s no right method and wrong method in absolute terms. There are different choices for different situations. But to make those choices you first have to free yourself from the dogmas. And maybe consider that there are alternatives to excessive compression through techniques of controlled expansion.
Implant tapping: myths and reality
And while we’re at it, let’s also debunk the myth of tapping as a technique to “reduce compression.”
Tapping reduces insertion torque — that’s true. But it does not reduce overall bone compression. It simply moves the compression earlier, making it happen with the tapping instrument instead of with the implant.
The bone is still pushed, deformed, partly microfractured. When the implant then arrives, it finds a bed already prepared with less resistance, so it turns more easily. But the compression all happened. You just didn’t “feel” it in your fingers during final insertion.
This distinction is fundamental, because many colleagues use tapping thinking they’re being more conservative, when in reality they’re simply changing the timing of compression without changing its magnitude.
Evidence-based implantology: beyond the dogmas
You might wonder why I bother taking apart established certainties and confronting you with uncomfortable truths.
The answer is simple: because implant dentistry deserves better. It deserves clinicians who think, who question, who don’t passively accept what they’re told.
Every time I place an implant, I know I’m compressing bone. I know this compression will create zones of temporary resorption. I also know that in the right zones new bone will form.
And I know the final result will depend on the dynamic balance between these processes, influenced by implant design, surface, surgical protocol, and the characteristics of the patient’s bone. After osseointegration, then, osseoperception will also occur — the process through which the patient learns to “feel” again through the bone.
This awareness doesn’t make me technically better. But it makes me more intellectually honest. And in a profession where fashions change every five years while the laws of physics stay immutable, intellectual honesty is worth more than any trendy technique.
The future of implantology
…lies in personalized protocols
The truth is, we’re only at the beginning.
The interaction between osteotomy protocol, implant design, surface, and bone characteristics is still a largely unexplored territory.
We oversimplified, for too long. And now the time has come to return to complexity, to make peace with the fact that easy answers are usually the wrong ones too.
In the next articles I’ll keep digging.
Keep questioning. Keep offering you a vision of implantology that isn’t content with prepackaged truths.
We’ll talk about how these concepts translate into concrete clinical choices, what implications they carry for loading timing, and how to truly personalize protocols instead of following standardized recipes.
But above all, I’ll keep telling you what others don’t have the courage to say.
Because you deserve to know. And your patients deserve to be treated by someone who thinks with their own head.
Don’t miss the next articles
If what you’ve read made you reflect, made you angry, or simply made you curious, you can’t afford to miss what comes next. Subscribe to the blog and get straight to your inbox the articles that dismantle the certainties of modern implantology.
Zero spam, zero sales. Only content that makes you think and genuinely improves your clinical practice.
The Bonebenders community is made of professionals who aren’t content with easy answers. If you’ve made it this far, you’re probably one of us.
You don’t agree? Comment at the bottom of the page. I’m all for freedom of thought and speech. Long live freedom.
Article freely inspired by the work “From Friction Stability to Osseointegration and all things in-between” published on Mattheos.net. Thanks to the authors for stimulating these critical reflections on implant mechanics.
References
- Razaghi N, Gill T, Patankar A, Petrie A, Shahdad S. Significance of Primary Stability in Nonimmediately Loaded Dental Implants: A Systematic Review and Meta-analysis. Int J Prosthodont. 2025;38(4):457-482. doi:10.11607/ijp.9115 · PMID: 40172942
- Tisci A, Fanelli F, Caponio VCA, Zhurakivska K, Dioguardi M, Troiano G. Resonance Frequency Analysis and Clinical Outcomes in Implant Dentistry: A Systematic Review and Meta-Analysis. Clin Implant Dent Relat Res. 2026;28(3):e70156. doi:10.1111/cid.70156 · PMID: 42117690
- Darriba I, Seidel A, Moreno F, Botelho J, Machado V, Mendes JJ, Leira Y, Blanco J. Influence of low insertion torque values on survival rate of immediately loaded dental implants: A systematic review and meta-analysis. J Clin Periodontol. 2023;50(2):158-169. doi:10.1111/jcpe.13733 · PMID: 36217696
- Putra RH, Cooray U, Nurrachman AS, Yoda N, Judge R, Putri DK, Astuti ER. Radiographic alveolar bone assessment in correlation with primary implant stability: A systematic review and meta-analysis. Clin Oral Implants Res. 2024;35(1):1-20. doi:10.1111/clr.14195 · PMID: 37840388
References retrieved from PubMed. The systematic reviews and meta-analyses cited confirm the article’s thesis: the threshold numbers of primary stability (torque, ISQ) are not validated predictors of clinical outcome.
References
Looking for a specialist?
Implantologia a Frosinone →Impianti dentali, carico immediato e rigenerazione ossea
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stai valutando un impianto dentale?
Ho scritto una guida in 8 capitoli che spiega tutto quello che un paziente dovrebbe sapere prima di sedersi in poltrona. Niente marketing — solo fatti, casi studio e una checklist per fare le domande giuste.
Scarica la guidaStay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment