Wang A1-C3 Alveolar Bone Classification: Beyond Misch D1-D4
In brief — The Wang A1-C3 classification separates cortical thickness and trabecular density as independent, measurable parameters, generating nine real bone configurations instead of the four theoretical ones of Misch. This quantitative system enables precise ridge expansion planning and clearly distinguishes between the mechanical difficulty of the procedure and surgical risk.
Sintesi (IT) — La classificazione Wang A1-C3 separa spessore corticale e densità spongiosa come parametri indipendenti, generando nove configurazioni ossee reali invece delle quattro teoriche di Misch. Un sistema quantitativo che permette una pianificazione precisa dell’espansione crestale e distingue la difficoltà meccanica dell’intervento dal rischio chirurgico.
For thirty years we lived with an empirical classification disconnected from reality. Thanks to modern radiographic technology, we can finally change it.
The traditional classifications of alveolar bone density, indispensable for planning implant surgery, started from a theoretical assumption that almost never materialises in clinical practice.
Looking at a preoperative CBCT, we found ourselves facing situations that Lekholm and Zarb or Misch failed to represent in their theoretical schemes.
The study by Wang and colleagues (from Taiwan) published in 2023 in BMC Oral Health finally gave scientific dignity to what many of us saw on tomographic sections and knew from practical experience.
Analysing 315 implant sites with precise quantitative measurements, these researchers demonstrated that crestal cortical thickness and trabecular density are completely independent parameters.
There is no significant correlation between the two, and this radically changes how we have to think about implant planning.
In our specific Bonebenders world, the perspective shifts entirely when we consider ridge expansion with expanders.
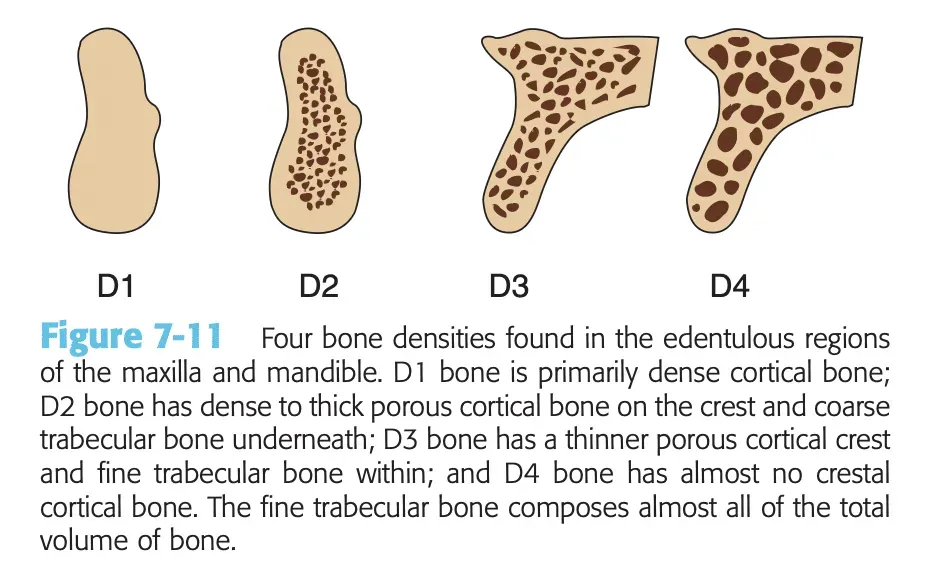
Let’s be clear. Expanding a D1 bone as represented by Misch is impossible. But how many true D1s do you know? Patients affected by osteopetrosis?
Wang’s Matrix System: Nine Possibilities Instead of Four
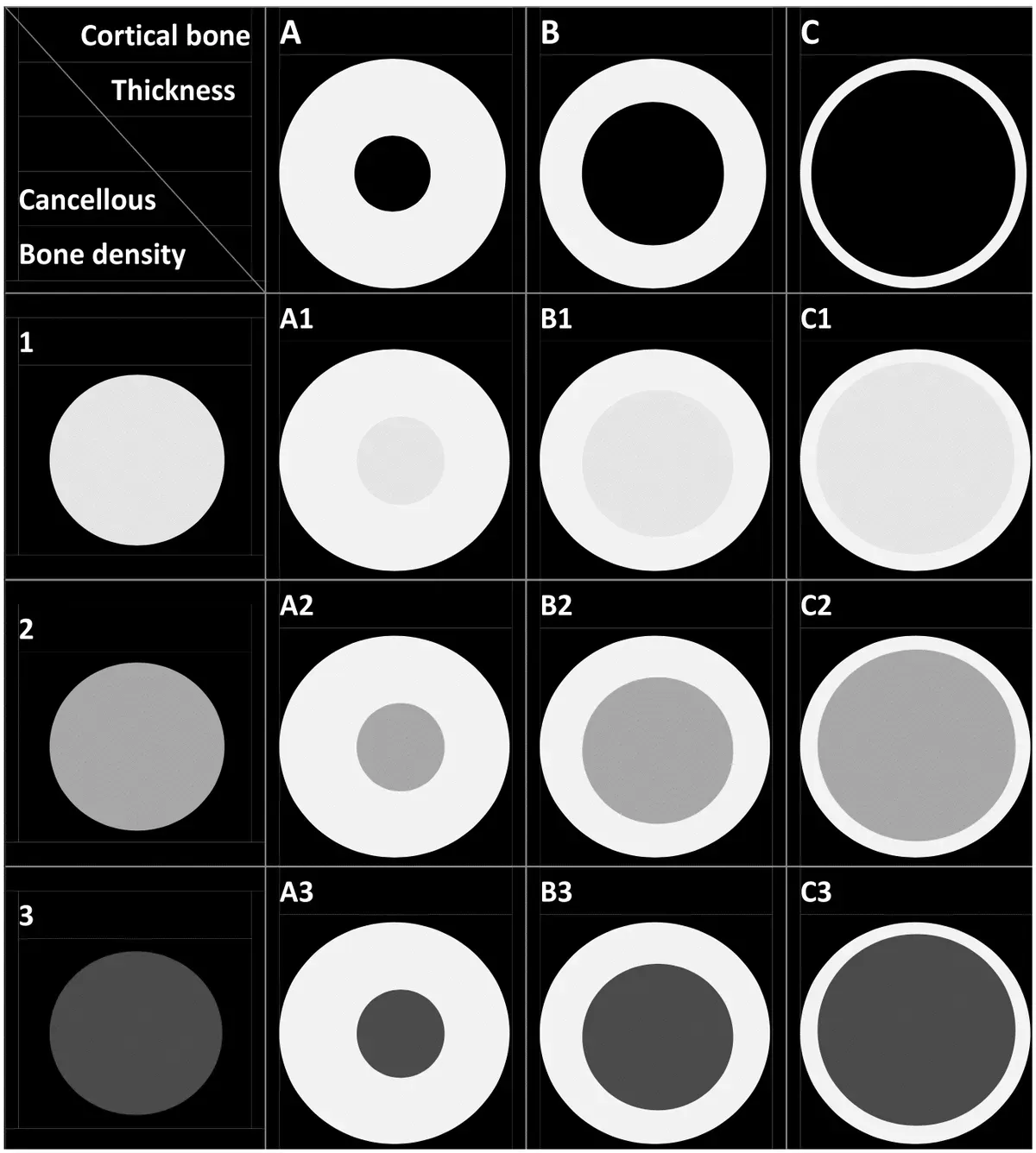
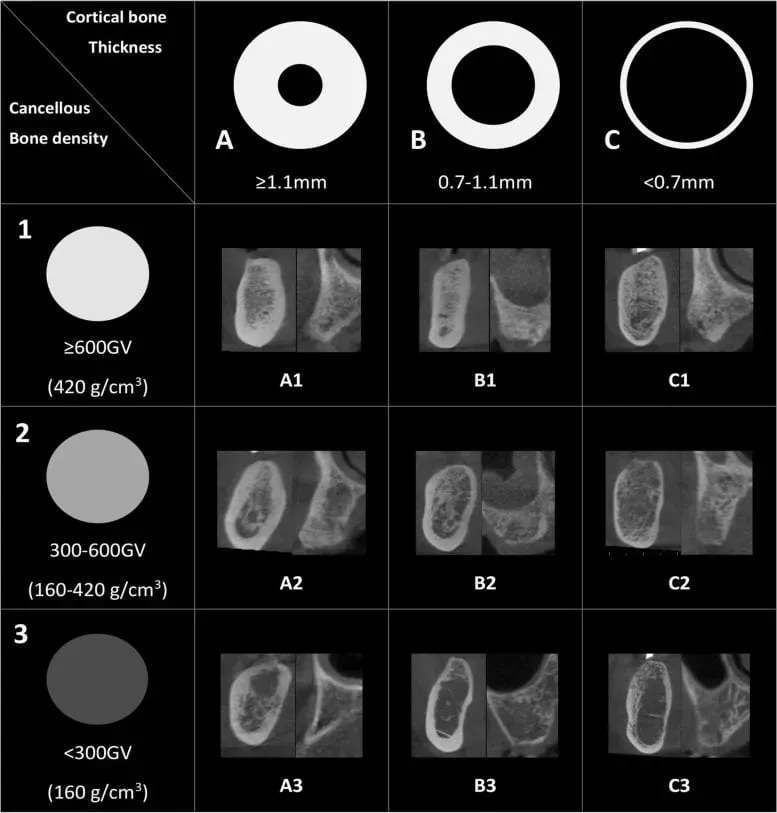
Wang’s quantitative classification explicitly separates the two bone components, cortical and trabecular, and measures them precisely. Crestal cortical bone is classified into three categories based on thickness: type A above 1.1mm, type B in the 0.7-1.1mm range, type C below 0.7mm.
Trabecular bone, on the other hand, is assessed by radiographic density on CBCT, with type one representing values above six hundred grayscale value (equivalent to four hundred and twenty grams per cubic centimetre), type two in the range between three hundred and six hundred, and type three for values below three hundred.
The combination of these two independent classifications generates a matrix of nine possible bone configurations, from A1 to C3. What makes this system revolutionary is not only the quantitative precision, but the fact that it includes and scientifically validates combinations that were previously considered anomalies, or not considered at all.
And instead, they are the reality we all see in the field.
Type A3, with a thick cortex but rarefied trabecular bone, represents over 4% of all implant sites. Type C1, with a thin cortex but dense trabecular bone, represents another 4.5%.
These are real situations we encounter regularly. They correspond to what we see on CBCT sections and are immediately recognisable and classifiable.
Compared with the D1-D4 classification the difference is abysmal. It is, at last, a leap into the everyday reality of implant dentistry, one that concretely helps the clinician find the right reference points.
I am not the only one to feel this need. A scoping review by Palomino-Zorrilla and colleagues, published in 2024 in the Journal of International Society of Preventive & Community Dentistry, combed through the systems used to describe bone before an implant and found an uncomfortable problem: most authors still adopt Lekholm and Zarb or Misch without ever having validated their diagnostic accuracy or inter-observer reproducibility. We classify bone, essentially, with rulers nobody has calibrated. The authors’ conclusion is blunt: we need a system built on the real characteristics of the tissue, with described, verifiable measurement methods. That is exactly the gap Wang fills.
Mechanical Difficulty Versus Surgical Risk
When we plan a ridge expansion, Wang’s classification gives us two crucial pieces of information that must be kept clearly distinct: how difficult it will be to mechanically expand the bone and how risky it will be to do so without complications. They are two completely different parameters.
Trabecular density and cortical thickness determine the mechanical difficulty of expansion — that is, how much we will have to weaken the wall and in what way to guide the expansive force, and how we will have to apply it.
Type A1 bone, with thick cortex and dense trabecular bone, is the hardest to expand of all. It requires meticulous preparation with diamond discs to strategically weaken the cortex, graded sequences of expanders, and above all patience. The high density opposes significant mechanical resistance and reduces elasticity.
You must never force the instruments, but rather understand how to help them overcome obstacles while maintaining the correct direction.
Each step requires time and controlled force. Yet it is precisely this structural robustness that makes it, in a sense, the safest: dense, thick bone forgives errors, it doesn’t fracture easily during manoeuvres if the operative sequence is followed rigorously and without forcing.
A colleague who already did expansion with the mallet in the upper arch once told me that in the lower arch she preferred GBR. Now, with expanders, she has changed her mind: expansion is her first choice for regeneration even in the mandibular arch.
I myself discovered, looking at my own statistics, that I do a greater number of lower expansions.
So, in fact, I prefer A1, A2 and B1 bone.
Type A1 is concentrated mainly in the posterior mandible (59% of cases).
In any case, A1 bone is operable with the Bonebenders kit. A hypothetical Misch D1 would, on the contrary, be inoperable.
And here the thick cortex becomes an ally, not an enemy. A systematic review by Al-Juboori and colleagues in 2024 in the Journal of Oral & Maxillofacial Research, across 418 implants, confirmed that regions with thicker cortical bone offer superior primary stability, with higher insertion torque and ISQ values at placement. Translated into our language: type A bone not only forgives errors during expansion, it also gifts that initial anchorage which makes the difference when immediate loading is on the table.
Bone types A2, B1 and B2 together represent 58% of all implant sites and constitute the ideal territory for expansion. They offer that perfect balance between workability and structural safety. Type B2 in particular, which alone represents over 20% of all sites, is the perfect starting point for those developing competence in the technique: manageable enough not to require excessive force, robust enough to forgive small imprecisions.
Type A3 presents an interesting dynamic. The thick cortex guarantees that structural stability which prevents fractures, while the rarefied trabecular bone allows a surprisingly easy expansion once the initial cortical barrier is overcome.
The key becomes under-preparation during implant insertion to exploit the osseodensification effect.
The screw expanders of our system are particularly effective in these cases because the pressure they exert compacts bone laterally and apically, compensating for the lower initial density of the trabecular component.
Type C Bone
Type C bone represents the exact opposite in terms of surgical dynamics. When cortical thickness drops below 0.7 millimetres, we find ourselves facing bone that lets itself be moulded easily.
Type C3, with thin cortex and rarefied trabecular bone, represents the worst-case scenario from the density standpoint. We find it in eighty-five percent of cases in the posterior maxilla.
It is easy to expand mechanically but it must also be densified to increase the initial stability of implants. Bonebenders expanders are ideal for not wasting a single gram of bone: they widen and densify.
The principle is not a workshop invention. A systematic review by Fontes Pereira and colleagues in 2023 in the Journal of Clinical Medicine gathered the evidence on osseodensification and documented that lateral compaction of bone increases peri-implant density, primary stability and bone-implant contact, precisely in narrow ridges and low-density zones like the posterior maxilla. The screw expanders work on the same viscoelastic mechanism: they don’t drill, they compress. Where Misch saw only a D4 to fear, we see a C3 to densify.
Like the colleague above, type C bone is what Bonebenders use at the start. You are excellent, but expansion is done in denser bone too.
Practical Implications for the Surgical Protocol
Quantitative classification serves not only planning but concretely guides execution.
With type A1, A2, B1 bone, at high density, we know we will have to invest more time in the osteotomy and preparation phase. Diamond discs become essential instruments for creating points of lower resistance that guide expansion in the desired direction.
This is necessary to avoid unwanted, uncontrolled fractures.
The sequence of expanders will have to be particularly gradual, with minimal increments between one diameter and the next. Patience becomes the implantologist’s main virtue.
But it doesn’t take much time. The sequences are fast.
With type C3, C2, B3 bone at low density, attention shifts entirely to the delicacy of the touch and to apical support. Expansion will be relatively easy, but precisely for this reason we must constantly restrain ourselves so as not to apply excessive force. The primary stability of the implant becomes critical, and under-preparation exploiting osseodensification is fundamental.
Beyond Numbers: A New Way of Thinking
What Wang’s classification has given us goes beyond categories and measurements. It has provided a common, quantitative and reproducible language to discuss clinical situations we could previously describe only subjectively. When a colleague tells me they treated a type B2 site instead of a generic D3-D4, I know exactly what we are talking about.
I can replicate their measurements on my own CBCT, compare our experiences on objective grounds, build that shared knowledge which truly advances the discipline.
For those who have worked with ridge expansion for years, this classification formalises and validates what experience had already taught.
For those approaching the technique, it provides a far more detailed map of the territory to explore, with one crucial distinction always present: hard bone does not necessarily mean risky bone.
Certainly, every case is different, but true D1s according to Misch are few. A true D1 cannot undergo expansion. But Wang A1 cases can.
This is a different category from the classic one of expansion: two distinct dimensions of the problem that we must learn to assess separately.
The next time you plan an implant, take the CBCT and measure: crestal cortical thickness in the central section of the site, trabecular density in the area that will host the implant. Classify the site according to Wang.
And if you decide to expand, ask yourself two separate questions: how difficult will it be to mechanically expand this bone, and how risky will it be to do so without complications. The answers to these two questions will guide your surgical preparation, the choice of instruments, the time you devote to the procedure, and above all the delicacy or assertiveness with which you will work.
Through all of this you must consider the most important matter: expansion is no longer what it was 40 years ago. It is all simpler, faster and more controllable. It is without doubt the fastest, most immediate and “simplest” regenerative method.
And the numbers hold up. A meta-analysis by Al Haydar, Kang and Momen-Heravi in 2023 in the International Journal of Oral & Maxillofacial Implants pooled 35 studies and over 4,400 implants: the ridge split produces on average about 3 mm of horizontal gain with a 98.2% implant survival rate, with or without grafting material. The figure that interests me most is precisely that last one: bone, when you guide it instead of replacing it, does the work itself. That is the heart of bonebending — and Wang finally gives us the map to know, site by site, how much to guide it.
The learning curve of these methods has flattened considerably, thanks to the Bonebenders kit.
❓ Frequently Asked Questions (FAQ)
What is the main difference between the Misch and Wang classifications?
The Misch classification (D1-D4) treats bone density as a single, theoretical parameter, while the Wang classification (A1-C3) separates cortical thickness and trabecular density as two independent variables measurable on CBCT. This generates nine real bone configurations instead of four theoretical ones, representing the clinical reality we face every day far better.
How do you measure bone density according to Wang on a CBCT?
Crestal cortical bone is measured in millimetres of thickness: type A above 1.1mm, type B between 0.7-1.1mm, type C below 0.7mm. Trabecular bone is assessed in grayscale value: type 1 above 600 GSV, type 2 between 300-600 GSV, type 3 below 300 GSV. Measurements are taken in the central section of the planned implant site.
Is type A1 bone too dense for ridge expansion?
No, A1 bone is workable with the correct technique. It requires more preparation with diamond discs to strategically weaken the cortex and graded sequences of expanders, but it is safer because it forgives errors. A true Misch D1 (which practically never exists in clinical reality) would be inoperable, but Wang A1 is a different, manageable configuration.
Which bone type is ideal for starting with ridge expansion?
Type B2 is perfect for those developing competence in the technique: it represents over 20% of all implant sites, manageable enough not to require excessive force yet robust enough to forgive small imprecisions. Types C2 and C3 are also relatively easy to expand, but require particular attention to primary stability.
How does the surgical protocol change between type A and type C bone?
With type A bone (thick cortex) you need diamond discs to create points of lower resistance, graded sequences of expanders and more time. With type C bone (thin cortex) expansion is mechanically easier but requires a delicate touch, implant under-preparation and particular attention to primary stability through osseodensification.
Where are the different bone types most frequently found?
Type A1 is concentrated mainly in the posterior mandible (59% of cases). Type C3 is found in 85% of cases in the posterior maxilla. Types A2, B1 and B2 together represent 58% of all implant sites and are distributed across both arches.
Does the Wang classification completely replace the traditional one?
Yes, for those doing ridge expansion the Wang classification is far more useful because it provides precise, reproducible quantitative parameters. It clearly separates the mechanical difficulty of expansion (trabecular density + cortical thickness) from surgical risk, allowing much more accurate planning of the operative protocol.
References
- Wang S-H, Hsu J-T, Fuh L-J, Peng S-L, Huang H-L, Tsai M-T. New classification for bone type at dental implant sites: a dental computed tomography study. BMC Oral Health. 2023;23(1):324. doi:10.1186/s12903-023-03039-2 · PMID: 37231447
- Palomino-Zorrilla JJ, Córdova-Limaylla NE, Rosas-Díaz JC, Cayo-Rojas CF, Cervantes-Ganoza LA, Guerrero ME. Jawbone quality classification in dental implant planning and placement studies. A scoping review. J Int Soc Prev Community Dent. 2024;14(2):89-97. doi:10.4103/jispcd.JISPCD_4_22 · PMID: 38827351
- Al-Juboori H, Petronis Z, Razukevicius D. The interrelation between cortical bone thickness and primary and secondary dental implant stability: a systematic review. J Oral Maxillofac Res. 2024;15(4):e2. doi:10.5037/jomr.2024.15402 · PMID: 40017687
- Fontes Pereira J, Costa R, Nunes Vasques M, Salazar F, Mendes JM, Infante da Câmara M. Osseodensification: an alternative to conventional osteotomy in implant site preparation: a systematic review. J Clin Med. 2023;12(22):7046. doi:10.3390/jcm12227046 · PMID: 38002660
- Al Haydar B, Kang P, Momen-Heravi F. Efficacy of horizontal alveolar ridge expansion through the alveolar ridge split procedure: a systematic review and meta-analysis. Int J Oral Maxillofac Implants. 2023;38(6):1083-1096. doi:10.11607/jomi.9972 · PMID: 38085739
FAQ
- What is the main difference between the Misch and Wang classifications?
- The Misch classification (D1-D4) treats bone density as a single, theoretical parameter, while the Wang classification (A1-C3) separates cortical thickness and trabecular density as two independent variables measurable on CBCT. This generates nine real bone configurations instead of four theoretical ones, representing the clinical reality we face every day far better.
- How do you measure bone density according to Wang on a CBCT?
- Crestal cortical bone is measured in millimetres of thickness: type A above 1.1mm, type B between 0.7-1.1mm, type C below 0.7mm. Trabecular bone is assessed in grayscale value: type 1 above 600 GSV, type 2 between 300-600 GSV, type 3 below 300 GSV. Measurements are taken in the central section of the planned implant site.
- Is type A1 bone too dense for ridge expansion?
- No, A1 bone is workable with the correct technique. It requires more preparation with diamond discs to strategically weaken the cortex and graded sequences of expanders, but it is safer because it forgives errors. A true Misch D1 (which practically never exists in clinical reality) would be inoperable, but Wang A1 is a different, manageable configuration.
- Which bone type is ideal for starting with ridge expansion?
- Type B2 is perfect for those developing competence in the technique: it represents over 20% of all implant sites, manageable enough not to require excessive force yet robust enough to forgive small imprecisions. Types C2 and C3 are also relatively easy to expand, but require particular attention to primary stability.
- How does the surgical protocol change between type A and type C bone?
- With type A bone (thick cortex) you need diamond discs to create points of lower resistance, graded sequences of expanders and more time. With type C bone (thin cortex) expansion is mechanically easier but requires a delicate touch, implant under-preparation and particular attention to primary stability through osseodensification.
- Where are the different bone types most frequently found?
- Type A1 is concentrated mainly in the posterior mandible (59% of cases). Type C3 is found in 85% of cases in the posterior maxilla. Types A2, B1 and B2 together represent 58% of all implant sites and are distributed across both arches.
- Does the Wang classification completely replace the traditional one?
- Yes, for those doing ridge expansion the Wang classification is far more useful because it provides precise, reproducible quantitative parameters. It clearly separates the mechanical difficulty of expansion (trabecular density + cortical thickness) from surgical risk, allowing much more accurate planning of the operative protocol.
References
Looking for a specialist?
Rigenerazione Ossea a Frosinone →Il Metodo Bonebenders: espansione osteo-mucosa senza innesti
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stai valutando un impianto dentale?
Ho scritto una guida in 8 capitoli che spiega tutto quello che un paziente dovrebbe sapere prima di sedersi in poltrona. Niente marketing — solo fatti, casi studio e una checklist per fare le domande giuste.
Scarica la guidaStay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment