«But don't you perforate the membrane?» Almost never: the sinus in three dimensions
In brief — Many colleagues picture sinus floor elevation as a vertical move: go up, perforate the membrane, fill the void. That is the logic of someone planning on a sheet of paper. On a CBCT you work in space: the floor cortex is expanded and repositioned across all three planes, the membrane stays intact and rises with the bone. You only perforate to engage the apex when stability demands it — a 3 mm lift at most, relying on the tent effect of the expanded cortex. No graft, single stage.
Sintesi (IT) — Molti colleghi pensano il rialzo di seno come un gesto verticale: salire, bucare la membrana, riempire. È il ragionamento di chi progetta su un foglio di carta. Sulla CBCT si lavora nello spazio: la corticale del pavimento si espande e si riposiziona nei tre piani, la membrana resta integra e sale con l’osso. Si buca solo per ingaggiare l’apice quando serve stabilità — sollevamento massimo 3 mm, effetto tenda della corticale espansa. Senza innesto, in una sola seduta.
The wrong question
«But you put nothing into the transcrestal lift? And you don’t perforate the membrane? And then, the implant apex sits in the sinus».
I get these every time. They are honest questions, asked by good clinicians. But they all spring from the same error of perspective: they picture the surgery as if it happened on a single plane. On a sheet of paper.
It’s understandable. The periapical radiograph is two-dimensional. The panoramic is two-dimensional. For decades we read bone on a flat surface, and on a flat surface there is only one useful direction: up. If you have little bone and the sinus is low, the only move the sheet allows you is to go up. Going up means reaching the membrane. Reaching the membrane means perforating it. Perforating means filling.
The problem isn’t the reasoning. The problem is the sheet.
Space has three planes, not one
I don’t plan on the sheet. I plan on the CBCT. And the CBCT is not a more detailed radiograph: it is a different geometry. It shows me the ridge across the three planes of space — bucco-palatal, mesio-distal, apico-coronal — and in three planes the available moves are not one, they are many.
I can recruit bone laterally, where nature left it, and expand it toward the point where it’s needed. I can open the buccal cortex and move it. I can take the bony floor of the sinus and relocate it where I decide, not where the sheet forces me to go. This is what bonebending means: bone is not a block to drill through, it is a living tissue that bends and shifts. The technique grows from there, from the ridge expansion of Scipioni and my father, and in the sinus it takes a precise name.
My father called it Localized Management of Sinus Floor. LMSF. It was 1998, the International Journal of Oral & Maxillofacial Implants, with Scipioni, Calesini and myself.¹ Four hundred and ninety-nine implants, 303 patients, 97.5% survival in ridges with 5–7 mm of residual bone. No window was opened. The cortex was expanded and the sinus floor was elastically lifted, from the crest, in the same session as the implant.
The membrane is a passenger, not a target
Here is the point the sheet cannot show. In the vast majority of cases — say 99% — I do not reach the Schneiderian membrane at all.
I move the cortex of the floor. The membrane rests on top of it and rises with it, whole. Between my instrument and the ciliated epithelium there is always bone. It isn’t an elevation of the membrane: it is a repositioning of the bone, and the membrane travels as a passenger. That’s why “perforating it” is not the rule — it’s the exception.
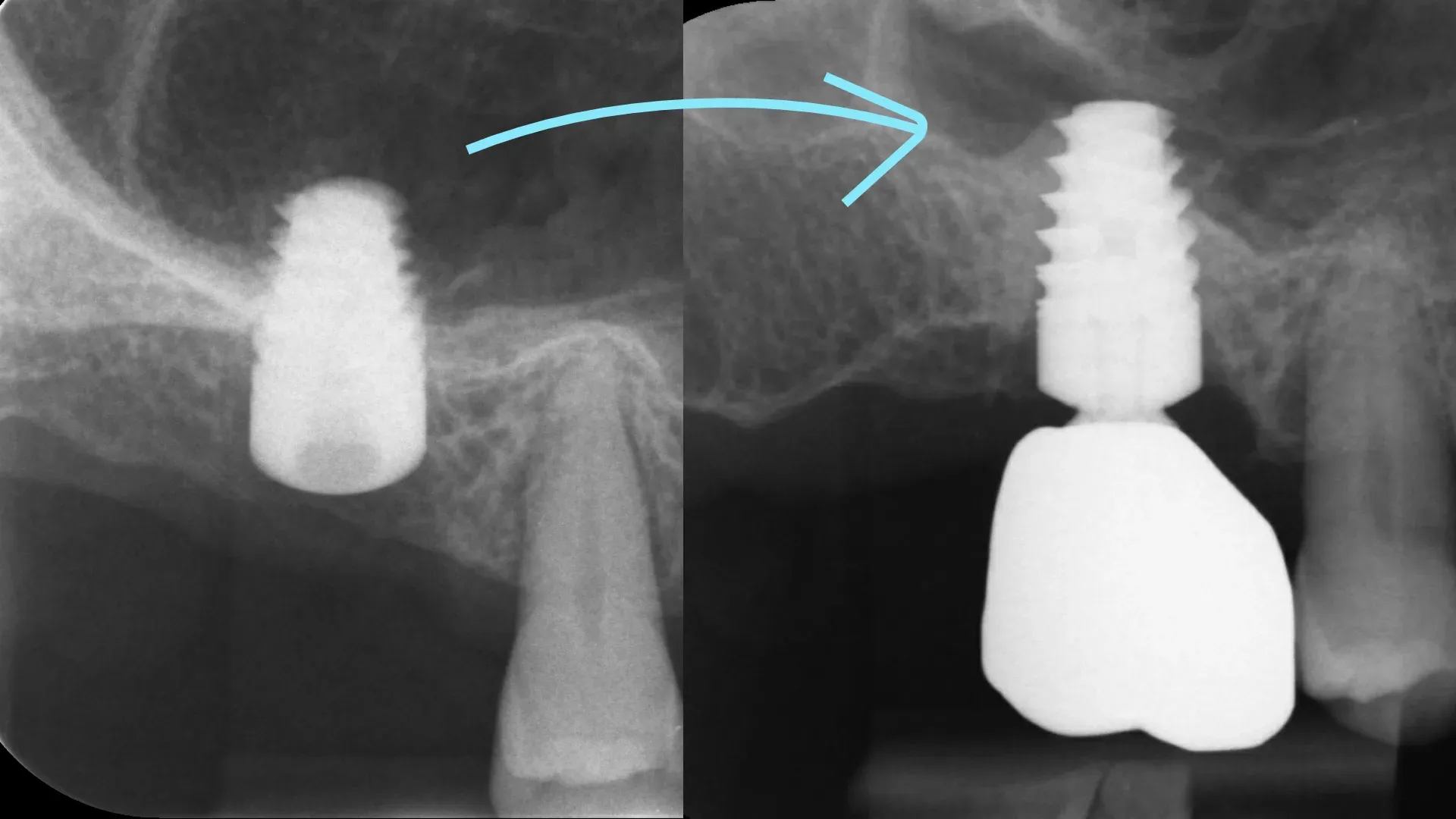
The exception exists, and it must be stated. When I don’t need to lift much but I need more primary stability, then yes: I perforate in a controlled way and engage the implant apex beyond the cortex. But there the lift is minimal, 3 mm at most, because I am not relying on the implant to hold the space open: I rely on the tent effect of the expanded apical cortex. The expanded cortex acts as the pole, the apex stabilises it, the membrane stretches over it like the canvas of a tent, and bone forms beneath. It is the same biology Lundgren documented in 2004:⁵ membrane lifted, no graft, and bone forms all the same, by the principle of guided tissue regeneration. I told it step by step in a graftless LMSF clinical case.
Two scenarios, then. In neither do I “go up and fill”.
«It won’t heal that way». It heals that way.
I know what the colleague reasoning in two dimensions thinks: without biomaterial, that space won’t ossify. He is wrong, and it isn’t my opinion.
Winter and Odrich — Ronald Odrich, one of the mentors I learned from in New York — took the LMSF and applied it to ridges with less than 4 mm of residual bone, mean 2.87 mm.² They lifted an average of 9 mm, with no graft and no covering membrane. Survival 91.4%. Their phrase stuck: osseointegration occurs through an endosteal–periosteal continuum, free from the need for a graft to resorb. Translated: the biomaterial, there, is a guest that slows things down, not an ally you need.
The follow-up says the rest. In post-extraction molar sites, at nearly ten years on average, LMSF gave 100% survival, with both vertical and horizontal expansion of the bone.³ And the contemporary flapless version, published in Heliyon in 2021, confirmed 95% using only native bone: the osteotomes directed first toward the cortex of the medial wall, then redirected for the final osteotomy.⁴ No particulate. No window.
Feel free not to believe me. The numbers are public.
What changes for you
If you reason on the sheet, facing an atrophic ridge you see two roads: the lateral window with a graft, or giving up. If you reason in space, you see a third, often the shortest: expand what is there and relocate it, in a single session, without importing what isn’t.
It is not magic and it is anything but universal. When the ridge is too low to stabilise the implant, when the membrane is diseased, when there is active sinus disease, or when the anatomy clearly calls for the lateral window — you change technique, without romanticism. But “not enough bone” almost never means what it seems to mean on the sheet. Far more often it means that no one has yet looked at the case in the three planes where it actually exists.
The difference is not in the instrument. It is in the number of dimensions you allow yourself to think in.
References
- Bruschi GB, Scipioni A, Calesini G, Bruschi E. Localized management of sinus floor with simultaneous implant placement: a clinical report. Int J Oral Maxillofac Implants 1998;13(2):219-26. PubMed
- Winter AA, Pollack AS, Odrich RB. Placement of implants in the severely atrophic posterior maxilla using localized management of the sinus floor: a preliminary study. Int J Oral Maxillofac Implants 2002;17(5):687-95. PubMed
- Bruschi GB, Crespi R, Capparè P, Bravi F, Bruschi E, Gherlone E. Localized management of sinus floor technique for implant placement in fresh molar sockets. Clin Implant Dent Relat Res 2013;15(2):243-50. DOI · PubMed
- Bruschi GB, Bruschi E, Papetti L. Flapless Localised Management of Sinus Floor (LMSF) for trans-crestal sinus floor augmentation and simultaneous implant placement. A retrospective non-randomized study: 5-year of follow-up. Heliyon 2021;7(9):e07927. DOI · PubMed
- Lundgren S, Andersson S, Gualini F, Sennerby L. Bone reformation with sinus membrane elevation: a new surgical technique for maxillary sinus floor augmentation. Clin Implant Dent Relat Res 2004;6(3):165-73. PubMed
FAQ
- So you really put nothing into the transcrestal sinus lift?
- In most cases, nothing. The space created beneath the lifted cortex and around the implant apex fills with a clot, which is invaded by osteoblasts and mineralises. It is the same mechanism as a post-extraction socket. Lundgren and colleagues demonstrated it back in 2004: the elevated membrane and the implant are enough to form bone, with no biomaterial.
- But don't you perforate the Schneiderian membrane?
- Almost never. In the order of 99% of cases I don't even reach it: I move the cortex of the sinus floor, and the membrane sits on top, intact, and rises with it. I perforate only when I need more stability and have to engage the implant apex — and in that case I lift no more than 3 mm, relying on the tent effect of the expanded cortex.
- If the implant apex protrudes into the sinus, isn't that a problem?
- It depends how much and how. An apex protruding a few millimetres under an intact, taut membrane, with no sinus disease, is exactly the pole holding up the biological tent. It becomes a problem when it tears the membrane, when the anatomy is unfavourable, or when primary stability is lacking. Case selection is everything.
- Do you work with osteotomes, expanders, under-preparation?
- With calibrated screw expanders and, depending on the case, magnetodynamic-percussion osteotomes. I under-prepare the site and place the implant simultaneously, from the crest, with no lateral window. The logic is not to drill upward: it is to expand the native cortex and relocate it where it is needed.
- Why should I trust this technique over GBR or the lateral window?
- You don't have to trust me. Look at the numbers. The original 1998 series reported 97.5% across 499 implants. The independent validation by Winter and Odrich in New York in 2002, in ridges with less than 4 mm of residual bone, reported 91.4%. Follow-up at nearly ten years in post-extraction molar sites: 100% survival. When the anatomy calls for a lateral window, though, the lateral window is done. The tool follows the case, not the habit.
References
Looking for a specialist?
Implantologia a Frosinone →Impianti dentali, carico immediato e rigenerazione ossea
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stai valutando un impianto dentale?
Ho scritto una guida in 8 capitoli che spiega tutto quello che un paziente dovrebbe sapere prima di sedersi in poltrona. Niente marketing — solo fatti, casi studio e una checklist per fare le domande giuste.
Scarica la guidaStay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment