Guiding Healing Rather Than Chasing Regeneration: Maxillary Rehabilitation Following Bonebenders Principles
Guest post by Dr. Dario Tuscano
Tooth loss is not always the consequence of acute infectious processes or traumatic events. Far more often, in daily practice, we face patients with advanced periodontitis: progressive resorption of the supporting tissues, mobility, pathological migration, functional and aesthetic compromise.
In these cases the clinician faces a choice that defines the entire treatment plan. Simply replace the lost teeth — or design a rehabilitation that preserves and makes the most of the residual biological capital. The case I present stems from this second line of thinking and represents a practical application of the Bonebenders philosophy.
The initial situation

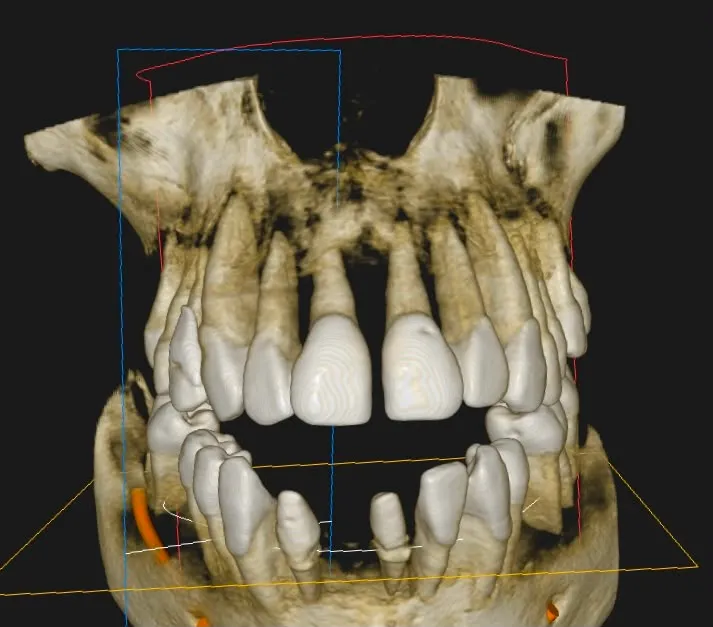
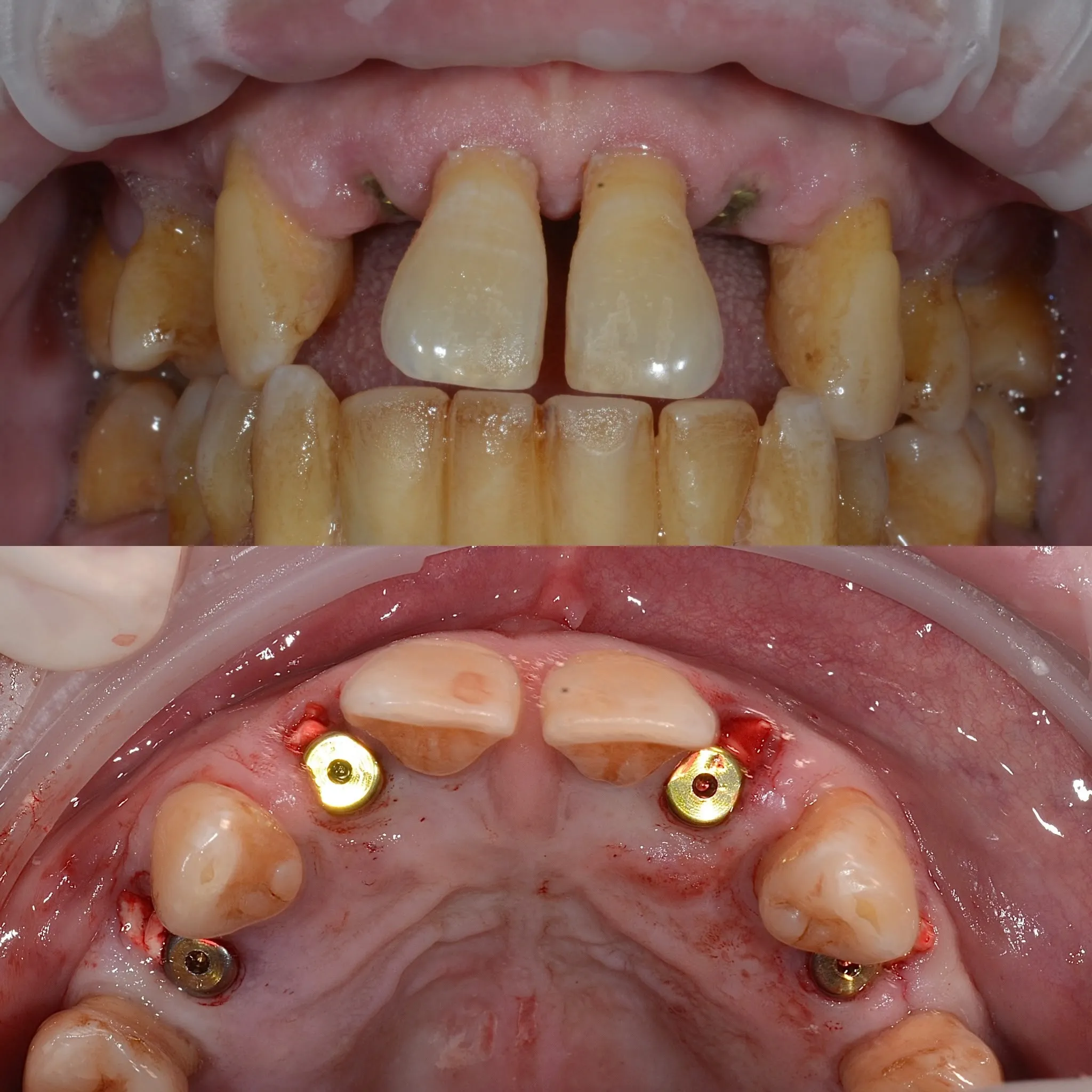
The patient presented with severe periodontal compromise affecting almost all teeth. Despite years of supportive periodontal therapy, the remaining elements showed:
- severe loss of bone support
- vestibular migration
- advanced gingival recessions
- high mobility
- marked dentinal hypersensitivity
This last aspect was the main reason for the visit: the patient reported pain even from the simple passage of air during breathing. From a prognostic standpoint, the affected teeth were no longer able to guarantee stable masticatory function over time.
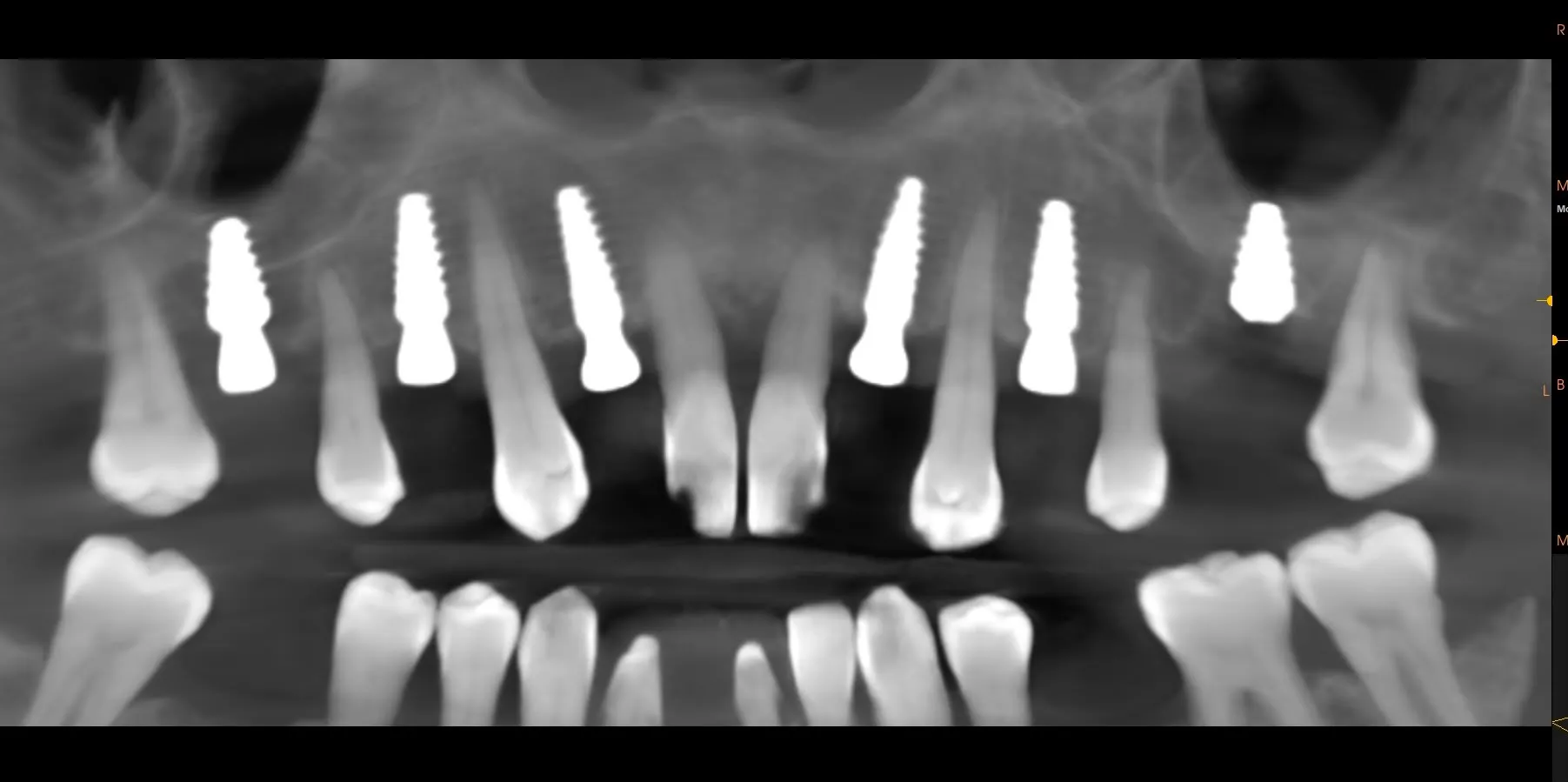
The surgical phase: post-extractive implants and bone expansion
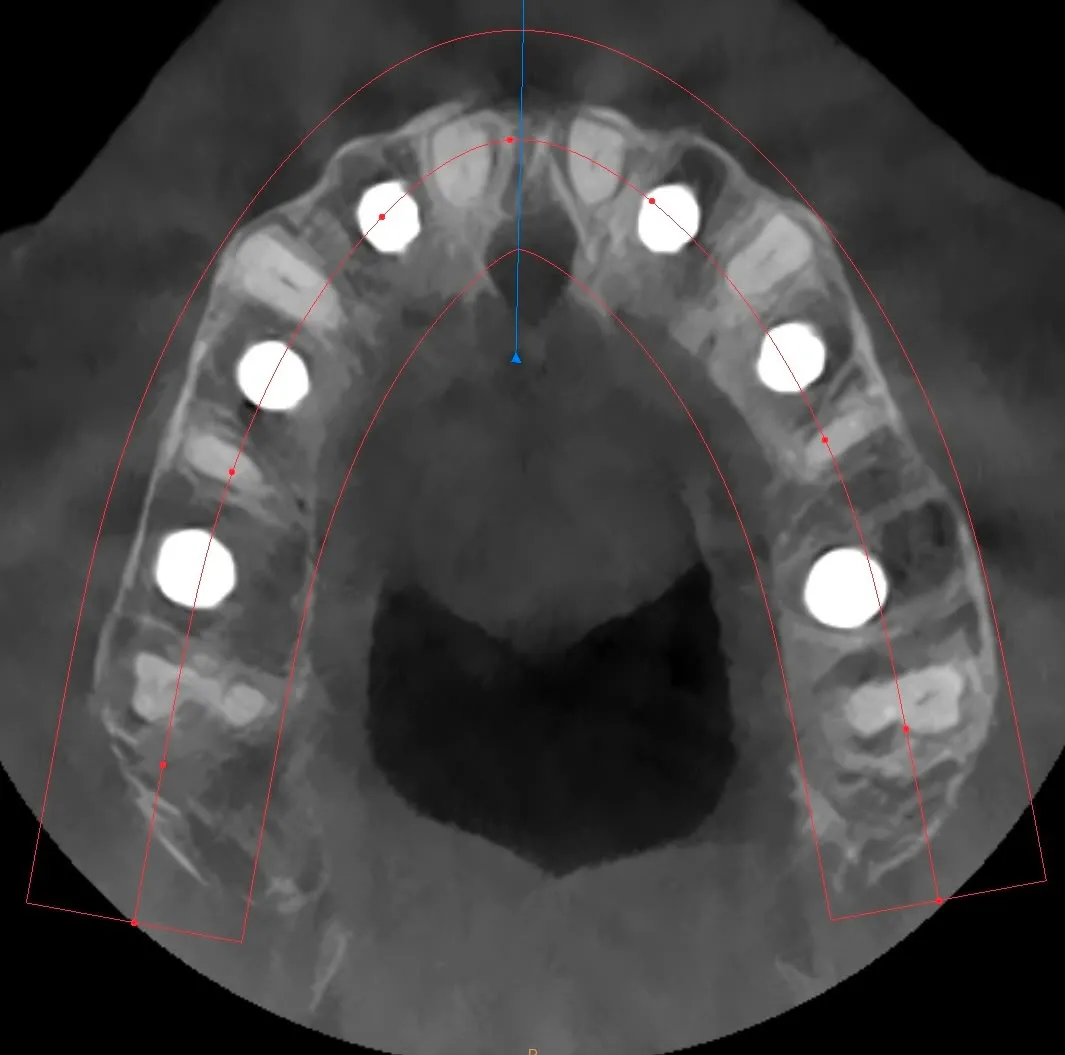
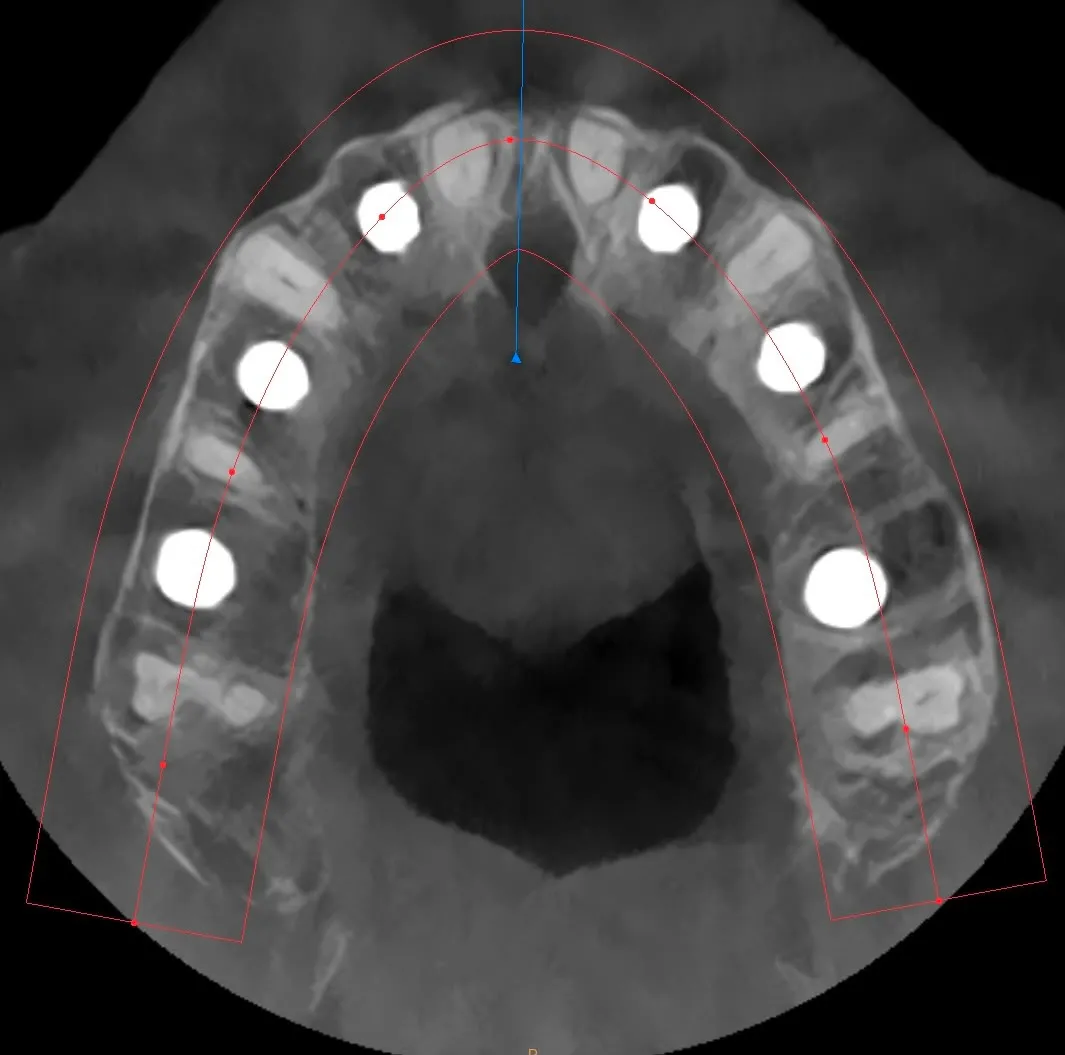
After extraction of the compromised teeth (12, 14, 22, 24 and 26), six immediate post-extractive implants were placed at positions 1.6 – 1.4 – 1.2 – 2.2 – 2.4 – 2.6.
In the anterior post-extractive sites, implant placement was carried out by engaging the palatal wall of the sockets using the lancet drill designed by Dr. Bruschi. This choice made it possible to:
- move the implant away from the vestibular cortex
- preserve vestibular bone thickness
- exploit the residual bone structure
- achieve correct prosthetic emergence
- promote soft tissue stability over time
The LMSF technique at site 1.6
Site 1.6, where the ridge had already healed, was treated using the LMSF technique with the bone expanders from the Bonebenders kit.
The atraumatic elevation of the Schneider membrane and simultaneous bone distraction — a gentle and controlled displacement of the bone structure present at the palatal recess in a palato-vestibular direction — allowed simultaneous implant placement while avoiding more invasive procedures such as a traditional sinus lift.
Apical expansion at site 2.6
In this case the post-extractive implant was combined with a crestal sinus lift performed through the residual socket.
The implant was stabilised by engaging the sinus cortex and elevating the residual bone structure without placing or requiring resorption of any biomaterial at the treated site. The controlled expansion of the apical bone and the gentle elevation of the sinus membrane using the expanders designed by Dr. Bruschi achieved what he himself has called “Apical Expansion”.
This phenomenon exemplifies how biomechanical manipulation of bone can stimulate regenerative processes by harnessing the biological capacity of tissues to adapt and remodel.
Why I did not raise flaps
A fundamental principle of the Bonebenders philosophy is respect for vascularisation and the regenerative capacity of the periosteum.
Peri-implant tissues derive from the masticatory mucosa which, expressing itself in reparative mode, covers and seals the breach in the organism’s integrity represented by the implant with a junctional epithelium. Implant healing should be considered a cicatricial-reparative phenomenon. Every time we raise a mucoperiosteal flap we interrupt part of the blood supply from the periosteum — and in a context that requires perfusion and oxygen, this inevitably reduces healing capacity.
Hence the rationale for maintaining periosteal perfusion during the surgical phases — by not raising flaps or by using split-thickness flaps instead of full-thickness ones. Minimally invasive access and split-thickness flaps allow us to preserve:
- tissue vascularisation
- the contribution of periosteal stem cells
- local regenerative potential
The goal was not simply to place implants, but to create the ideal biological conditions for their integration.
Managing the provisional: the strategic role of remaining teeth
An often-underestimated aspect of these cases is management of the transitional phase. Some teeth were temporarily retained as abutments for a fixed provisional, leaving implant healing undisturbed.
This allowed the patient to keep their smile, maintain adequate function, avoid a removable prosthesis and face the treatment journey without significant social impact. Only after biological maturation of the implants were the remaining teeth extracted.
Some elements (17 and 27) were still maintainable, and this represented a significant biological and biomechanical advantage. Although the phenomenon of so-called osseoperception exists, the mechanical sensitivity of implants remains inevitably inferior to that provided by a natural tooth. In this specific case, the posterior teeth continued to provide proprioceptive feedback throughout all treatment phases, allowing the patient’s neuromuscular system to retain important occlusal control mechanisms.
This aspect takes on even greater importance — and is, in my opinion, often overlooked — in modern implant-prosthetic rehabilitations made in zirconia.
Soft tissue conditioning

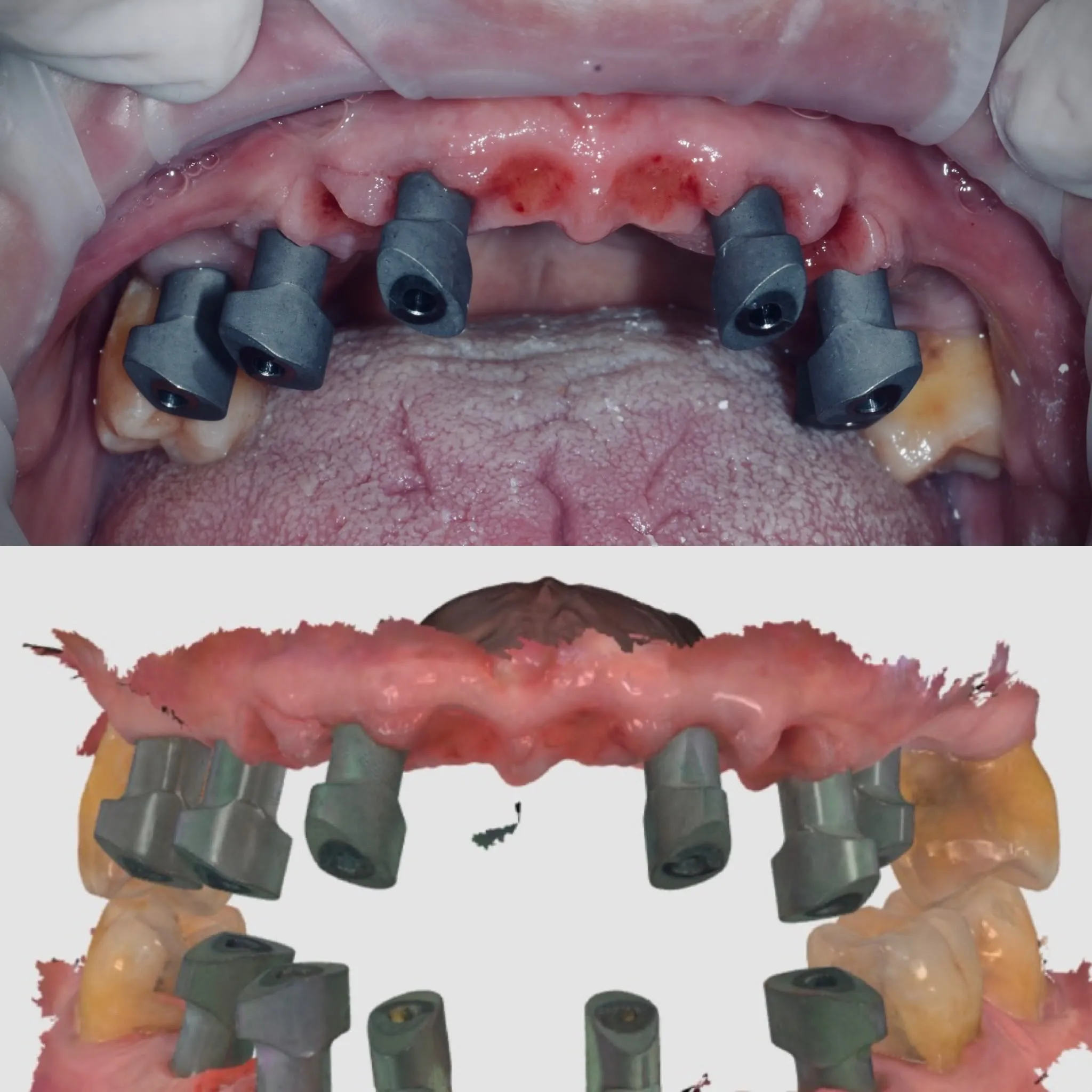
After the second surgical stage a provisional supported exclusively by the implants was delivered. At the post-extractive sites no complex regenerative materials were used: only collagen sponges were placed.
Tissue stability was achieved primarily through correct prosthetic design. The pontics were shaped to extend approximately 3–3.5 mm below the gingival margin, guiding healing and controlled tissue collapse.
The clinician’s goal is not to force healing, but to guide it. When implantology respects biology, biology returns stability.

Conclusions

This case demonstrates that managing severely compromised patients does not necessarily require extensive regenerative procedures or aggressive resective approaches. The key to success lies in understanding biological principles:
- respect for vascularisation
- correct three-dimensional implant positioning
- preservation of vestibular bone walls
- judicious use of bone expansion
- proper prosthetic management of soft tissues
The Bonebenders philosophy reminds us that implantology is not simply about replacing missing teeth, but about creating the conditions for tissues to heal and remain stable over time.

FAQ
Is it possible to rehabilitate a severely compromised maxilla without bone grafting or extensive surgery?
What is the LMSF technique and how does it work?
Why avoid full-thickness flaps in implant surgery?
What role do remaining teeth play during the provisional phase?
Go deeper
Espansione crestale (split crest) →Allargare la cresta senza trapianto — tecnica ERE e bonebending
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stai valutando un impianto dentale?
Ho scritto una guida in 8 capitoli che spiega tutto quello che un paziente dovrebbe sapere prima di sedersi in poltrona. Niente marketing — solo fatti, casi studio e una checklist per fare le domande giuste.
Scarica la guidaStay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment