In brief — Francesco’s story: tooth extractions during military service to avoid conscription, then decades of defective prosthetics and compromised bridges. A rebirth through regenerative bonebending that rebuilt the lost alveolar bone, giving him back natural teeth and dignity.
The boy who lost his smile
Francesco was just a boy when he was called up for military service. He was good-looking, blond, with light eyes. And he had a bright smile, full of life.

He would gladly have avoided the army. Girls courted him, he had already found a good job. To him it looked like a waste of precious time.
One day Francesco ran into the village dentist on the street and, chatting about this and that, he mentioned this worry of his to “the doctor”. And the doctor did not let the chance slip: “Come to me. I’ll pull a few teeth. They’ll declare you unfit for service, and then I’ll put them back nicer than before!”
And that is how our Francesco lost his upper incisors.
Unfortunately, the army doctor who examined him afterwards noticed the recent extractions and the warped logic behind them. Francesco was a physically impressive young man and soon became a good soldier — even without teeth.
After the three months of recruit training, he was posted to a barracks in Cuneo. Here his life took an unexpected turn, thanks to meeting a kind-hearted military physician who set out to find a solution for his problem. With the few means available, he built him a removable denture with clasps — a simple device that improved his quality of life, let him eat almost normally again, and gave back a semblance of normality and a sense of autonomy he thought he had lost for good.
Francesco felt like a prisoner in the barracks. He couldn’t wait to get back to his life.

When he could finally go home, he went straight to find the “doctor” who had promised to fix the mutilation with teeth “nicer than before!”. And the nicer-than-before teeth were a fixed bridge anchored to the remaining teeth.
For some years Francesco wore that bridge, then a second one, because some of the abutment teeth holding up the first were hit by secondary decay. By that point all of Francesco’s upper teeth were bridges or crowns (“caps”) in gold and resin.
Over time he realised what a poor choice had been made back in his army days.
The encounter and the rebirth
When I examined him — by now retired, with grown children — he told me the whole story from the beginning, with regret. He was ashamed and unhappy with his situation: the bridge had been repaired countless times, no longer held reliably, and the aesthetics were beyond saving. I remember reassuring him that I had already successfully treated people with a similar history — because I had. What’s more, Francesco is a man of uncommon vitality, and I was certain that fixing his teeth would mean a true rebirth for him. I could already picture him with new teeth and a renewed ease with people.
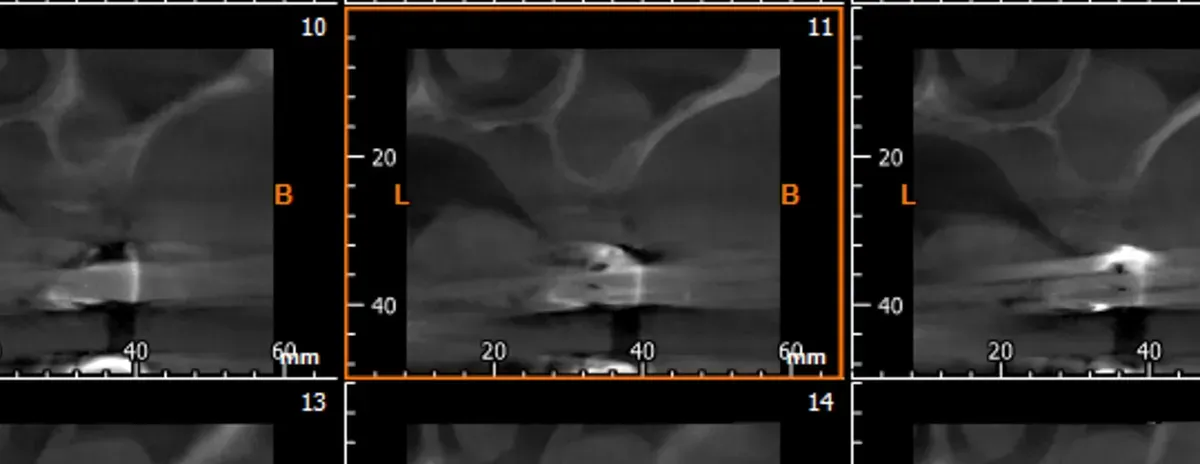
Technically, the problem was finding fixed pillars to rest the new restoration on. Traumatic extractions and time had thinned the residual bone — the bone you need to anchor titanium implants — down to a frail, too-slender structure. And in the posterior sectors, recurring infections of the now hopelessly ruined teeth had shrunk the alveolar bone both vertically (below the maxillary sinus) and horizontally (on the cheek side).
This was one of those cases many colleagues call “severely atrophic”, a term meant to signal the absence of adequate bony anchorage for implants. Yet that label is used far too often to justify approaches that are effective but very invasive. Truly “severely atrophic” cases are few, and in many of them a regenerative approach by expansion is preferable. And that is what I did for Francesco.
I told him: “Don’t worry. Give me a little of your time and you’ll come back as good as new. Life has its own way of renewing us, of letting us start over and giving us new chances. And I’ve been given the gift of meeting you, so I can show you it’s possible.”
The result
Six months later, Francesco had solved his problem. Eight years have passed now, and we only see each other for the periodic check-ups with me and the dental hygienist. And he is very good at his home hygiene maintenance.
These are the real satisfactions of our work.

If you are a colleague interested in the technical aspects of the work done with Francesco, you can join our community by following the link at the bottom of the page!
What the research says
For years the word «atrophy» sounded like a sentence. It isn’t.
The systematic review with meta-analysis by Al Haydar and colleagues (International Journal of Oral & Maxillofacial Implants, 2023), built on 35 studies and 4,446 implants, measured a 98.2% implant survival rate after ridge expansion. But the figure that really interests me is another one: the horizontal bone gain — about 3 mm — was identical with or without grafting material. Bone, when you treat it with respect, regenerates on its own. That is exactly the logic of bonebending: open a space and let the patient’s own blood fill it.
A second meta-analysis confirms it, the one by Lin and colleagues (BMC Oral Health, 2023): 3.3 mm of gained width and 98.1% survival. Numbers that stand up against far more aggressive techniques.
And here lies the point that divides clinicians. Vorovenci and colleagues (Biomedical Reports, 2024) compared expansion, osseodensification and guided bone regeneration: GBR gains on average 4.0 mm, expansion 3.7 mm. A tiny difference, against a procedure that is less invasive, faster, with a single surgical stage. For a man like Francesco — a full life, eager to get straight back to eating and talking — those few tenths of a millimetre are not worth months of waiting and the discomfort of a large graft harvested elsewhere.
The most recent evidence points the same way. A 2025 randomised controlled trial (Atef and colleagues, Clinical Implant Dentistry and Related Research) showed that the modified version of the technique reliably reconstructs even the atrophic posterior mandible, the trickiest zone. Case selection remains everything: not every ridge can be expanded, and the long-term outcomes depend on how much vital bone we manage to preserve. But when the conditions are there, expansion does something no block of bone harvested elsewhere can do: it gives back living, vascularised bone, already ready to integrate.
References
- Al Haydar B, Kang P, Momen-Heravi F. Efficacy of Horizontal Alveolar Ridge Expansion Through the Alveolar Ridge Split Procedure: A Systematic Review and Meta-Analysis. Int J Oral Maxillofac Implants. 2023;38(6):1083-1096. DOI · PMID: 38085739
- Lin Y, Li G, Xu T, Zhou X, Luo F. The efficacy of alveolar ridge split on implants: a systematic review and meta-analysis. BMC Oral Health. 2023;23(1):894. DOI · PMID: 37986181
- Vorovenci A, Drafta S, Petre A. Horizontal ridge augmentation through ridge expansion via osseodensification, guided bone regeneration and ridge-split: Systematic review and meta-analysis of clinical trials. Biomed Rep. 2024;21(4):139. DOI · PMID: 39161939
- Atef M, Shawky M, Mounir M, Gibaly A. Assessment of Modified Ridge Split With Autogenous Versus Xenogenic Augmentation: Randomized Clinical Trial. Clin Implant Dent Relat Res. 2025;27(3):e70046. DOI · PMID: 40342252
FAQ
When is regenerative bonebending appropriate in cases of severe atrophy?
How long does healing take with bonebending compared to traditional treatments?
Does the bone regenerated by bonebending stay stable over time?
What are the psychological advantages of bonebending for the patient?
References
- https://doi.org/10.11607/jomi.9972
- https://doi.org/10.1186/s12903-023-03643-2
- https://doi.org/10.3892/br.2024.1827
- https://doi.org/10.1111/cid.70046
- https://pubmed.ncbi.nlm.nih.gov/38085739/
- https://pubmed.ncbi.nlm.nih.gov/37986181/
- https://pubmed.ncbi.nlm.nih.gov/39161939/
- https://pubmed.ncbi.nlm.nih.gov/40342252/
Go deeper
Espansione crestale (split crest) →Allargare la cresta senza trapianto — tecnica ERE e bonebending
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stai valutando un impianto dentale?
Ho scritto una guida in 8 capitoli che spiega tutto quello che un paziente dovrebbe sapere prima di sedersi in poltrona. Niente marketing — solo fatti, casi studio e una checklist per fare le domande giuste.
Scarica la guidaStay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment