Myofibroblasts: what they are and why they decide whether an implant heals
In brief — Myofibroblasts are activated fibroblasts that, if uncontrolled, produce dense scar tissue around implants. When osteoblasts “lose the race” on the implant surface, myofibroblasts generate fibrointegration, which leads to implant failure even without infection. Implant surface quality, biomechanical strategies and emerging pharmacological approaches can steer cells toward osseointegration, not fibrosis.
Sintesi (IT) — I miofibroblasti sono fibroblasti attivati che, se incontrollati, producono tessuto cicatriziale denso attorno agli impianti. Quando gli osteoblasti “perdono la corsa” sulla superficie implantare, i miofibroblasti generano fibrointegrazione che causa il fallimento implantare anche in assenza di infezione. La qualità della superficie, le strategie biomeccaniche e gli approcci farmacologici emergenti possono guidare le cellule verso l’osteointegrazione.
The answer you don’t expect.
From quiescent to killer: how fibroblasts could sabotage your implants.
Medical implants have revolutionised modern medicine, improving and extending the lives of millions of patients worldwide. From cardiac pacemakers to orthopaedic prostheses, from breast implants to our own implants, these devices play a crucial role in treating countless conditions.
And yet, behind every implantology success hides a silent battle between our immune system and these “foreign bodies”.
Has it ever happened to you, fellow dentists, that:
- You had patients who inexplicably lost several implants, which became mobile in the absence of infection
- You thought that implant was placed really well and could not possibly fail… and yet…
- You removed implants that looked perfectly integrated, but were painful and surrounded by fibrous tissue with no infection
In such cases, according to the study examined in this article, the culprits could be myofibroblasts.
The Biocompatibility Dilemma
When an implant of any kind is inserted into our body, it inevitably triggers what is called the “foreign body reaction” (FBR). It is an evolutionary, protective response of our organism, designed to identify, isolate and reject any object recognised as foreign.
This defence mechanism, essential as it is for our survival, can compromise the function of medical implants and create serious clinical complications.
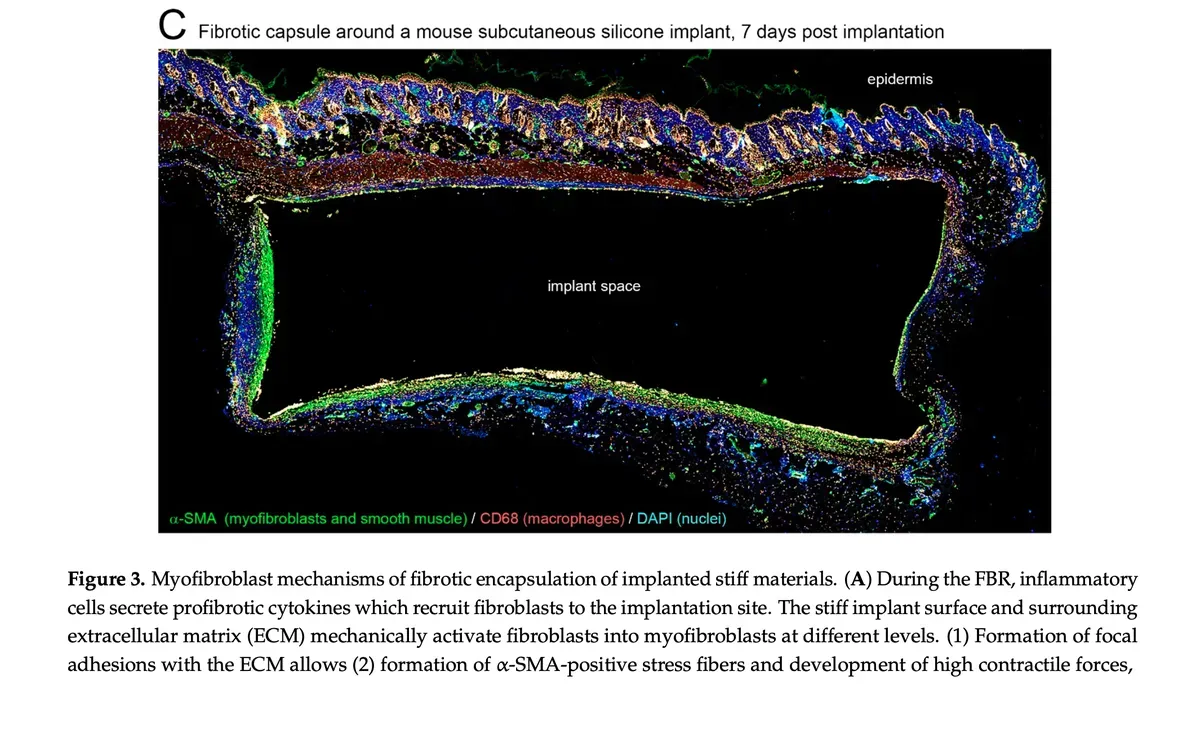
Noskovicova, Hinz and Pakshir of the Laboratory of Tissue Repair and Regeneration at the University of Toronto, in the article titled Implant Fibrosis and the Underappreciated Role of Myofibroblasts in the Foreign Body Reaction, express the following important concept:
“For the first time, we identified the precise molecular mechanism that turns normal healing into pathological fibrosis. And above all: we know how to stop it.”
The Clinical Consequences: When Implants Fail
Pacemakers and defibrillators require replacement every 10–15 years, with roughly 10,000–15,000 removal procedures worldwide each year. The fibrous tissue forming around these devices can make removal extremely risky because of scar adhesions.
Yet, even immersed in fibrous, scar tissue, those implants stay in place.
In our case, that process is called fibrointegration and it is not clinically acceptable, because it leads to failure. These implants do not hurt during healing (and sometimes even look healthy on radiographs), but they cannot bear load the moment the prosthetic part is connected, and they must be replaced, even without infection. It is a rare event compared with those above, but it exists and is best avoided as far as possible.
The Invisible Protagonists: what role might myofibroblasts play in this process?
At the centre of many implant-related complications sit precisely these specialised cells called myofibroblasts.
According to the study under review, they represent the missing link in understanding peri-implant fibrosis and have often been overlooked in previous research, which focused mainly on the role of macrophages.
But What Exactly Are Myofibroblasts?
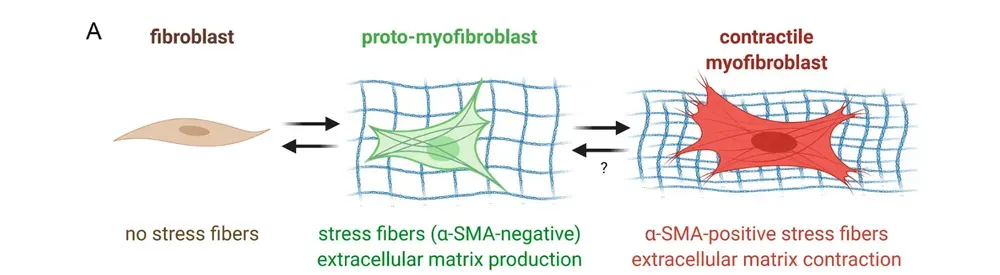
Myofibroblasts are fibroblasts “activated” by the healing/repair process that acquire characteristics similar to smooth muscle cells. They possess contractile ability and are responsible for producing collagen and other extracellular matrix components in the healing site.
Under normal conditions they help in wound healing, bringing the edges closer, but when activated excessively or chronically, they can form dense scar tissue around implants.
The Mechanism of Fibrosis and the Specific Case of Endosseous Implants
Fibrous tissue formation follows a complex cascade:
- Mechanical Activation: the rigid surfaces of implants mechanically stimulate fibroblasts
- Cellular Transformation: fibroblasts turn into contractile myofibroblasts
- Matrix Production: collagen and other structural proteins increase
- Capsule Formation: a dense fibrous capsule forms around the implant
In our specific case of dental implants, there is a competition between myofibroblasts and osteoblasts/osteocytes for colonising the implant surface. A decisive role belongs to the implant macro- and microgeometry, which steers the adsorbed proteins and then the cells one way or the other.
Osteoblasts/osteocytes slot in between phase 3 and phase 4, managing, in almost every case, to achieve osseointegration successfully, blocking phase 4 (fibrosis).
In essence, osteocytes win the race for the implant surface and start depositing bone matrix faster than fibroblasts can mature theirs.
The process is not that linear or simple, because the collagen matrix already laid down by fibroblasts is still needed by bone cells too, along with the protein matrix (proteome).
If, for various reasons, osteoblasts lose the match, the implant will fibrointegrate and then fail under load (or even before).
The event is rare, but it must be considered.
Innovative Strategies to Improve Biocompatibility
Surface Modifications
Researchers have developed several strategies to modulate the body’s response to implants:
Stiffness Control
Implants with softer surfaces (elastic modulus close to natural tissues) significantly reduce myofibroblast activation and fibrous tissue formation.
But this is not possible for dental implants, which are necessarily rigid and need a (semi-rigid) connection with the bone tissue they are immersed in.
Surface Topography
Surfaces with specific microtextures (features of 1–4 micrometres) can minimise inflammation and the foreign body reaction.
In this field, dental implants are very advanced, thanks to research on micro- and macrogeometries and on surface treatments, designed to favour the osteoblastic lineage over the fibroblastic one.
And recent research confirms that the race is won on the surface, in the first days. A 2024 RCT by Ko and colleagues (International Journal of Implant Dentistry) compared SLA implants with a hydroxyapatite nano-coating against uncoated SLA implants, placed immediately: by two, three and four months the coated implants showed significantly higher stability (ISQ). It is not a cosmetic detail. It is the timing that decides who colonises the titanium first, exactly in the window where myofibroblasts would try to take over. For anyone still attached to the old smooth surfaces, it is a figure worth pondering.
On the soft-tissue side the evidence is even more direct. Another RCT, Yossri and colleagues 2024 (Clinical Implant Dentistry and Related Research), treated abutment surfaces with cold plasma: compared with controls, inflammatory cells collapsed while organised collagen fibres, fibroblast adhesion and E-cadherin expression rose sharply. Translated: the right surface does not silence the fibroblastic response, it orders it. That is exactly the harmonious coexistence we are talking about here.
Two recent systematic reviews widen the picture in the same direction. Dai and colleagues (2025, Journal of Dentistry) conclude that cold atmospheric plasma improves osseointegration and soft-tissue healing together; Liang and colleagues (2023, Frontiers in Bioengineering and Biotechnology) document how bioactive-glass coatings on titanium increase osteogenesis, anti-inflammatory properties and soft-tissue adhesion. The thread is always the same, and it is worth stating plainly: don’t make the implant inert, make it a biological interlocutor.
Special Coatings
The use of low protein-adhesion materials, such as zwitterionic hydrogels, can reduce cell adhesion and biofilm formation. Feasible for dental implants?
Pharmacological Approaches
Several anti-fibrotic drugs are under study:
- Pirfenidone: already approved for pulmonary fibrosis, it has shown efficacy in reducing peri-implant fibrosis
- Integrin Inhibitors: they block the mechanical activation of TGF-β, a key factor in fibrous tissue formation
- Controlled Release: local delivery systems releasing anti-fibrotic drugs directly onto the implant surface
Here the most solid evidence comes, paradoxically, from breast surgery. A 2025 systematic review (Daronch and colleagues, Aesthetic Plastic Surgery) reviewed the drugs against capsular contracture — the fibrosis that imprisons breast implants — and finds old acquaintances: pirfenidone, leukotriene inhibitors, even tamoxifen, able to modulate myofibroblasts in the experimental capsule model. It strikes me every time: peri-implant fibrosis, wherever it happens, speaks the same molecular language. What we learn to stop around a breast implant tells us something about the titanium we put in bone too.
Conclusions: Toward a Harmonious Coexistence
Understanding the crucial role of myofibroblasts in the foreign body reaction opens new prospects for improving the biocompatibility of medical implants. It is no longer just about creating inert materials, but about designing surfaces and systems that “talk” constructively with our organism.
The ultimate goal must never be to completely eliminate the immune response — impossible and potentially dangerous — but rather to guide it toward a controlled healing response that favours implant integration without compromising function.
With an ageing population and the growing demand for implantable devices, research in this field becomes ever more crucial, aiming to truly minimise possible complications and make implants, dental and otherwise, ever more universally applicable.
In cases of significant bone deficits, where cellular competition becomes even more critical, applying tailored bone regeneration techniques can make the difference between implant success and failure.
This article is based on:
The cover image is taken from the original article, in compliance with the CC 4.0 licence.
Have you ever had a patient with an ‘unexplained’ failure?
Have you ever had an implant that looked radiographically perfect and then moved in the absence of infection?
Have you ever wondered why that implant you were so sure of didn’t make it?
To dig deeper into these themes, I recommend also reading our articles on second-intention healing and bone regeneration with PDL.
FAQ: Myofibroblasts and Fibrointegration
Q: What is the difference between osseointegration and fibrointegration?
A: Osseointegration is the direct bond between bone and implant: osteoblasts colonise the implant surface and lay down mineralised bone. Fibrointegration is the isolation of the implant by dense fibrous scar tissue. They can look similar on radiographs, but they are clinically opposite: osseointegration carries load, fibrointegration fails.
Q: Are myofibroblasts always harmful?
A: No. They are essential in the early healing phase to approximate wound edges and build the matrix bone needs. The problem arises when they stay chronically active, blocking osteoblasts from reaching the implant surface. It is a question of timing and of “who gets there first”.
Q: What determines the “winner” between osteoblasts and myofibroblasts?
A: Mainly three factors: implant micro- and macrogeometry, surface treatment, and the biological quality of the recipient site. These steer the adsorbed proteins and then the cells toward the osteoblastic or the fibroblastic lineage. Significant bone defects increase the risk of fibroblastic dominance.
Q: Is fibrointegration preventable?
A: Yes, in most cases. Thanks to the evolution of dental implant surfaces (microtextures, hydrophilic treatments) fibrointegration rates are rare. In sites with significant bone deficit, guided bone regeneration techniques further reduce the risk by boosting osteoblastic competition.
Q: Are there clinical warning signs before a fibrointegrated implant fails?
A: Unfortunately not in the asymptomatic phase. The implant can stay radiographically quiescent and subjectively painless for months or years. Failure emerges at prosthetic connection, when it is mechanically loaded. That is why it is critical to limit risk factors during insertion.
Q: Could anti-fibrotic drugs become part of clinical implant practice?
A: It is a fascinating frontier. Studies on pirfenidone and integrin inhibitors show potential, but we are still far from routine clinical use. Controlled local drug release directly onto the implant surface represents the next horizon, without systemic effects.
References
- Noskovicova N, Hinz B, Pakshir P. Implant Fibrosis and the Underappreciated Role of Myofibroblasts in the Foreign Body Reaction. Cells. 2021;10(7):1794. doi:10.3390/cells10071794 · PMID: 34359963
- Daronch OT, Palhares Neto AA, Viterbo F. Non-surgical Treatment and Prophylaxis of Capsular Contracture in Mammary Implants: A Systematic Review of Literature. Aesthetic Plast Surg. 2025;49(15):4295-4303. doi:10.1007/s00266-025-04879-9 · PMID: 40259064
- Ko YC, Lee D, Koo KT, Seol YJ, Lee YM, Lee J. A randomized controlled trial of immediate implant placement comparing hydroxyapatite nano-coated and uncoated sandblasted/acid-etched implants using a digital surgical guide. Int J Implant Dent. 2024;10(1):29. doi:10.1186/s40729-024-00549-8 · PMID: 38839621
- Yossri D, Kheir El Din NH, Afifi NS, Adel-Khattab D. Soft tissue response to titanium healing abutments treated by Er:YAG laser or plasma spray: a randomized controlled feasibility clinical study with SEM and histological analysis. Clin Implant Dent Relat Res. 2024;27(1):e13373. doi:10.1111/cid.13373 · PMID: 39410747
- Dai Y, Sui X, Huang S, Li Y, Wang B, Liu Z. The application of cold atmospheric pressure plasma in prosthodontics. J Dent. 2025;163:106141. doi:10.1016/j.jdent.2025.106141 · PMID: 41038374
- Liang J, Lu X, Zheng X, Li Y, Geng X, Sun K, et al. Modification of titanium orthopedic implants with bioactive glass: a systematic review of in vitro and in vivo studies. Front Bioeng Biotechnol. 2023;11:1269223. doi:10.3389/fbioe.2023.1269223 · PMID: 38033819
FAQ
- What is the difference between osseointegration and fibrointegration?
- Osseointegration is the direct bond between bone and implant: osteoblasts colonise the implant surface and lay down mineralised bone. Fibrointegration is the isolation of the implant by dense fibrous scar tissue. They can look similar on radiographs, but they are clinically opposite: osseointegration carries load, fibrointegration fails.
- Are myofibroblasts always harmful?
- No. They are essential in the early healing phase to approximate wound edges and build the matrix bone needs. The problem arises when they stay chronically active, blocking osteoblasts from reaching the implant surface. It is a question of timing and of "who gets there first".
- What determines the "winner" between osteoblasts and myofibroblasts?
- Mainly three factors: implant micro- and macrogeometry, surface treatment, and the biological quality of the recipient site. These steer the adsorbed proteins and then the cells toward the osteoblastic or the fibroblastic lineage. Significant bone defects increase the risk of fibroblastic dominance.
- Is fibrointegration preventable?
- Yes, in most cases. Thanks to the evolution of dental implant surfaces (microtextures, hydrophilic treatments) fibrointegration rates are rare. In sites with significant bone deficit, guided bone regeneration techniques further reduce the risk by boosting osteoblastic competition.
- Are there clinical warning signs before a fibrointegrated implant fails?
- Unfortunately not in the asymptomatic phase. The implant can stay radiographically quiescent and subjectively painless for months or years. Failure emerges at prosthetic connection, when it is mechanically loaded. That is why it is critical to limit risk factors during insertion.
- Could anti-fibrotic drugs become part of clinical implant practice?
- It is a fascinating frontier. Studies on pirfenidone and integrin inhibitors show potential, but we are still far from routine clinical use. Controlled local drug release directly onto the implant surface represents the next horizon, without systemic effects.
References
Looking for a specialist?
Innesto Osseo a Frosinone →Tipi di innesto, tecniche e indicazioni per ricostruire l'osso perduto
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stai valutando un impianto dentale?
Ho scritto una guida in 8 capitoli che spiega tutto quello che un paziente dovrebbe sapere prima di sedersi in poltrona. Niente marketing — solo fatti, casi studio e una checklist per fare le domande giuste.
Scarica la guidaStay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment