The Bone's Neural Network: The Osteocyte Connectome
In brief — The osteocyte connectome is the bone’s cellular communication network: osteocytes talk to each other through cytoplasmic extensions running inside canaliculi, coordinating remodeling and mechanical adaptation. It is essential for implant osseointegration — and recent work shows it can be disrupted by ageing, disease, and even hijacked by bacteria.
Sintesi (IT) — Il connettoma osteocitario è la rete di comunicazione cellulare dell’osso: gli osteociti dialogano attraverso prolungamenti citoplasmatici, coordinando rimodellamento e adattamento meccanico. È essenziale per l’osteointegrazione degli impianti, e può essere alterato da invecchiamento, malattia e infezioni.
The term connectome usually refers to the map of neural connections in the brain. Here, it describes the structural and functional connections between bone cells.
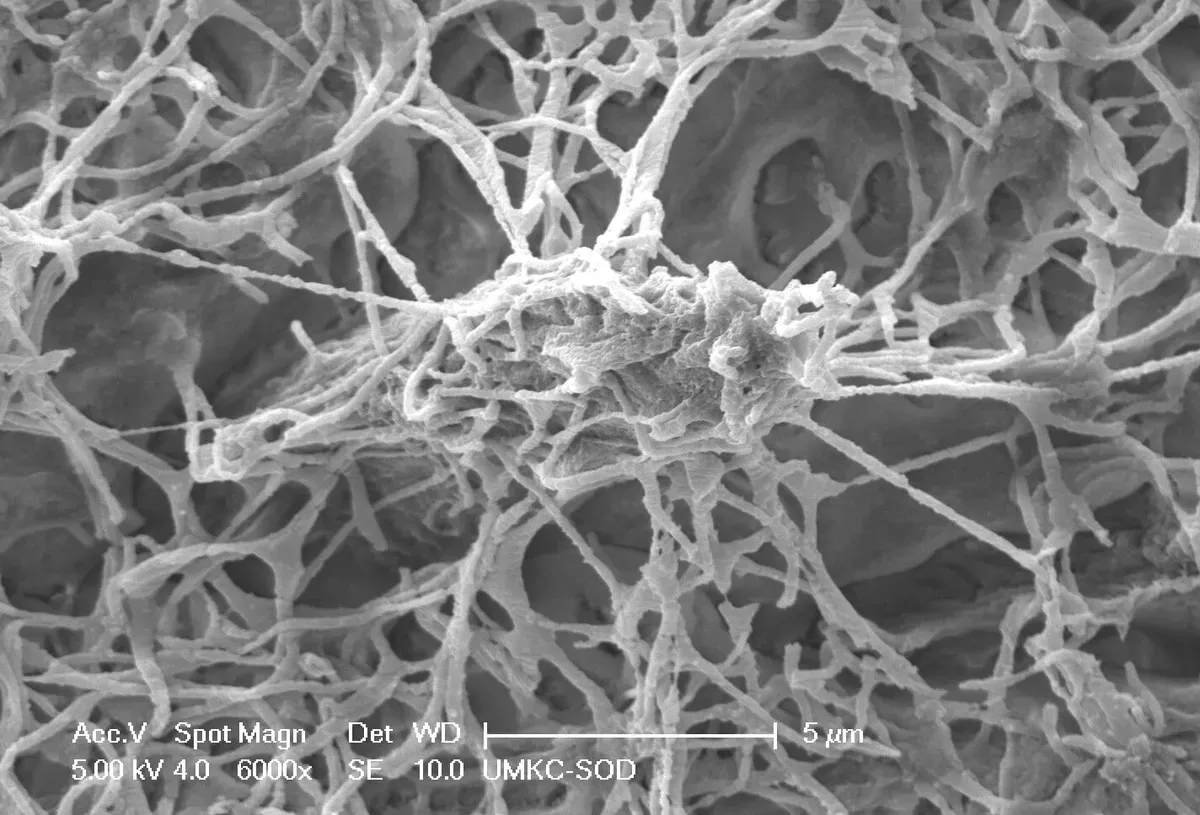
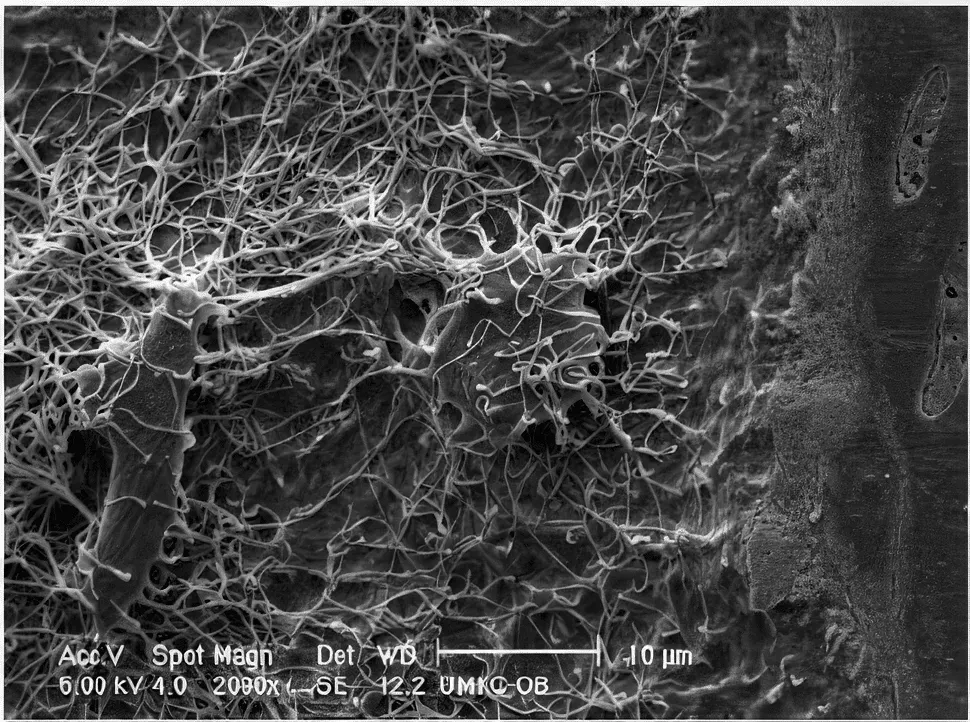
The paper titled Towards a Connectomic Description of the Osteocyte Lacunocanalicular Network in Bone examines the osteocyte network, focusing on the structure and function of the lacunocanalicular network (LCN) across various bone tissues. Osteocytes, the most abundant bone cells, form a complex network within bone tissue that is essential for skeletal health and mechanobiological adaptation. The detailed structure of this network — its connectome — had been studied far less, until recent advances in three-dimensional imaging.
Osteocytes sit inside bony lacunae, and their cytoplasmic extensions run through the corresponding canaliculi. It is obvious that osteocytes contact one another through these extensions. Yet the canalicular extracellular matrix is itself an integral part of the connectome and of the integrated osteocyte system.
Most of the osteocyte network’s functions can only be understood through the interaction between the intramembranous cellular network and the material inside the canalicular matrix.
Introduction and general observations on connectomics and network function
The paper introduces osteocytes and their network within compact bone tissue, highlighting their importance in cross-organ communication and bone remodeling.
As noted above, understanding the structure-function relationship in the osteocyte network can borrow methods developed in neural-network research. After all, the cellular processes of osteocytes recall the dendrites and axons of neurons.
The osteocyte network behaves like a bio-mechanical sensory organ. Beyond its obvious role in phosphate metabolism, this “organ” communicates with the kidney through Fgf23 and with the brain through leptin expression.
Osteocytes release various molecules — including osteocalcin, sclerostin and other osteokines — that can cross the blood-brain barrier and influence brain function.
Possible neuroprotective effects: Some studies suggest that osteocalcin, released by osteocytes, may have neuroprotective effects, positively influencing motor function and reducing neuronal loss and inflammation in the brain.
A 2025 review in Frontiers in Cell and Developmental Biology (Wu and colleagues) restates this view forcefully: the osteocyte is the conductor of skeletal homeostasis. It senses mechanical load through channels such as Piezo1 and through integrins, tunes the RANKL/OPG axis and the Wnt pathway via sclerostin, governs phosphate through FGF23. And when this cell falls ill — apoptosis, ferroptosis, pyroptosis — the lacunocanalicular network unravels and remodeling slips off its rails: this is the mechanism the authors place at the very core of osteoporosis. Worth one caution, though, raised by a 2023 review from Marahleh and colleagues: much of what we credit to the osteocyte comes from animal models that are not osteocyte-specific. Calling them “orchestrators” is evocative, but the clean, cell-by-cell evidence is in large part still missing.
Recent advances in imaging the LCN connectome
The paper outlines significant progress in imaging techniques — X-ray and electron microscopy — that have allowed better visualization of the LCN. Difficulties remain, however, because of the trade-off between resolution and field of view. Recent methods have improved the imaging of substantial portions of the network.
But seeing the network is not enough: what matters is how the fluid flows inside it. A 2023 multiphysics model (Boucetta and colleagues, J Mech Behav Biomed Mater) quantified fluid flow in the canaliculi and brought out a detail I find elegant — the redundancy of the interconnections keeps a partial flow alive even when microcracks appear. The network, put differently, is designed not to shut down at the first injury. And the same authors link this fluid flow to the regulation of osteoblasts, and therefore to the osseointegration of an implant.
The LCN connectome across different bone tissues
The paper shows how the connectome varies between bone-tissue types and between species. Studies report differences in osteocyte-network density and architecture between lamellar and trabecular bone, and between humans and other animals. These findings underline the potential of connectomic analysis to reveal fundamental aspects of bone biology and physiology.
How disease affects the LCN connectome
The paper describes how diseases such as osteoporosis and osteoarthritis can alter LCN architecture, affecting connectivity and, potentially, bone health. Quantitative studies are still needed to fully grasp the statistical significance and the implications of these changes.
And then there are the external enemies. A 2025 review in ACS Nano (Yi and colleagues) describes how Staphylococcus aureus exploits the lacunocanalicular network itself to invade cortical bone and hide from antibiotics: the connectome, from a highway of signals, becomes an escape route for the bacterium. It is one of the reasons chronic peri-implant infections are so stubborn — and why the shape and design of the implant matter as much as the technique used to prepare the site.
Ageing and the formation of the LCN connectome
The LCN connectome changes with age, affecting bone mechanosensitivity and overall health. Ageing is associated with reduced network density and connectivity, contributing to age-related bone loss. Understanding how the LCN forms and changes over time is fundamental to developing interventions aimed at maintaining or improving bone health.
There is an even finer level, and it sits inside the single cell. A 2025 review in Current Osteoporosis Reports (Jin and Nolte) places mitochondria at the heart of osteocyte mechanosensitivity: they reposition under load and — surprisingly — can even be transferred to neighbouring cells through membrane tunneling nanotubes and migrasomes. The network does not only exchange signals: it exchanges organelles. With age this traffic thins out, and with it the bone’s ability to adapt and to respond to the stimulus of an implant.
Conclusions:
Connectomic analysis of the osteocyte network is an emerging field that requires further research. The authors propose potential studies to clarify the function of the osteocyte network and its role in bone health. They suggest that understanding the LCN connectome could lead to new diagnostic tools for bone disease and to new therapeutic strategies, drawing on the study of neural and other biological networks.
Overall, the paper underlines the importance of understanding the LCN connectome for bone biology, highlighting the need for continued research and the potential benefits of interdisciplinary approaches in connectomics.
It is clear how essential the connectome is in surgical healing as well, particularly for implants. The same logic holds when we ask how implant macrogeometry and primary stability interact with the surrounding bone: it is the cellular network, not the single element, that coordinates repair.
❓ FAQ — The Osteocyte Connectome
🤔 What exactly is the osteocyte connectome?
The osteocyte connectome is the complete map of connections between osteocytes in bone, much like the neural connectome of the brain. Osteocytes communicate through cytoplasmic extensions that reach into the canaliculi, forming a lacunocanalicular network (LCN). This network enables cellular communication, nutrient exchange and the transmission of mechanical signals throughout the bone.
💬 How do osteocytes communicate with each other?
Osteocytes communicate through three main routes: 1) direct contact via gap junctions between their cytoplasmic extensions; 2) paracrine signaling by releasing molecules such as sclerostin and osteocalcin; 3) transport through the canalicular matrix. The network works as a “bone internet” to coordinate remodeling, repair and mechanical adaptation.
🔬 How does it differ from the nervous system?
Similarities: both are cellular communication networks with dendrite-like / axon-like extensions. Key differences: osteocytes are embedded in mineralized bone matrix, signal more slowly, are mainly mechanosensory, and also communicate with distant organs (kidney, brain) through hormones. The bone connectome is structurally stable yet functionally adaptive.
🎯 Why does it matter for implant dentistry?
The osteocyte connectome is fundamental to osseointegration. Osteocytes sense the presence of the implant, coordinate the reparative response and guide bone remodeling around the implant surface. An intact network favours better healing, while damage to the connectome (excessive surgical trauma, infection) can compromise integration. Respecting the osteocyte network is key to long-term success.
📉 How does it change with ageing?
With age, the osteocyte connectome undergoes progressive degeneration: fewer osteocytes, fewer cellular processes, loss of network connectivity. This impairs mechanosensitivity, slows remodeling and reduces reparative capacity. The result: more fragile, less responsive bone. In implant dentistry, this calls for gentler techniques and longer healing times in older patients.
🚫 What damages the osteocyte connectome?
Harmful factors include: excessive surgical trauma (overheating, excessive pressure), infection, radiotherapy, drugs such as bisphosphonates, prolonged immobilization, systemic disease (diabetes, osteoporosis). Smoking too compromises vascularization and cellular communication. Minimally invasive surgery and tissue respect protect the osteocyte network.
🔮 What does the future of research hold?
Future research aims at: complete 3D mapping of the human connectome, development of “connectome-friendly” biomaterials, therapies to regenerate the osteocyte network, early diagnosis of bone disease through connectivity analysis. Potential applications: implants that “dialogue” with the connectome, targeted drugs to restore connections, personalized medicine based on the individual connectomic profile.
🌱 How can we optimize regeneration while respecting the connectome?
Key strategies: atraumatic surgery with dedicated instruments, preservation of vascularization, respected healing times, gradual loading, adequate nutrition (vitamin D, protein). The Bonebenders techniques naturally respect the connectome: controlled distraction lets the network reorganize, healing by second intention preserves existing connections. Less trauma = a healthier network = better outcomes.
References
- Wu Y, Gan D, Liu Z, et al. Osteocytes: master orchestrators of skeletal homeostasis, remodeling, and osteoporosis pathogenesis. Front Cell Dev Biol. 2025;13:1670716. DOI · PubMed
- Marahleh A, Kitaura H, Ohori F, Noguchi T, Mizoguchi I. The osteocyte and its osteoclastogenic potential. Front Endocrinol (Lausanne). 2023;14:1121727. DOI · PubMed
- Jin J, Nolte PA. Mitochondrial distribution and osteocyte mechanosensitivity. Curr Osteoporos Rep. 2025;23(1):22. DOI · PubMed
- Boucetta A, Ramtani S, Garzón-Alvarado DA. Both network architecture and micro cracks effects on lacuno-canalicular liquid flow efficiency within the context of multiphysics approach for bone remodeling. J Mech Behav Biomed Mater. 2023;141:105780. DOI · PubMed
- Yi J, Chen Z, Li R, et al. Orthopedic implant infection management: prevention, barrier breakthrough, and immunomodulation. ACS Nano. 2025;19(30):27009-27032. DOI · PubMed
Acknowledgements: Heartfelt thanks to Elena Bozhikova for the valuable bibliographic contribution that made this in-depth piece possible.
References
Looking for a specialist?
Innesto Osseo a Frosinone →Tipi di innesto, tecniche e indicazioni per ricostruire l'osso perduto
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment