The “Revolutionary” Discovery of Hot Water
In brief — Second-intention healing has been used by great surgeons for over a century (Kazanjian, Tatum, Bruschi since 1998). A recent 2024 paper rediscovers it as “innovation”. In reality, peer-reviewed research proves the superiority of membrane-free guided healing in oral tissues.
Sintesi (IT) — La guarigione per seconda intenzione è stata usata dai grandi chirurghi per oltre un secolo (Kazanjian, Tatum, Bruschi dal 1998). Un recente paper 2024 la riscopre come “innovazione”. In realtà, la ricerca peer-reviewed dimostra la superiorità della guarigione guidata senza membrane nei tessuti orali.
The Principles of Second-Intention Healing: Historic Pioneers
Going further back, many well-known authors — pioneers of regenerative dentistry — had already introduced the concepts of second-intention healing and its countless advantages in implantology.
Two names deserve to be remembered above all:
VARAZTAD H. KAZANJIAN: the first maxillofacial surgeon, an Armenian immigrant to the United States, trained at Harvard and a field military surgeon in the First World War. He believed deeply in second-intention healing and devised the vestibuloplasty that bears his name and exploits these very principles.
HILT TATUM: American, devoted more to clinical practice than to academic career, he used second-intention healing extensively and devised the mini sinus lift and the split-crest.
It is clear, then, that this much-maligned approach has been used successfully by the finest surgeons since dentistry was born.
Regenerative Implantology: Research vs Clinical Vision
Scientific research in regenerative implantology has its own time, its protocols, its ethics committees, its peer review. And that’s fine.
But back in 1998, together with my father Gianni Bruschi and Dr. Scipioni, we were publishing on techniques for soft- and hard-tissue management that minimise surgical trauma in implantology; and in 1999 we documented bone and mucosal regeneration by second intention through tissue expansion — while some people still believed you always needed grafts and biomaterials…
…and, above all, primary-intention closure of the surgical wound.
Keratinized Tissue and Regeneration: The Scientific Truth for 26 Years
- Peri-implant tissues have an extraordinary intrinsic regenerative capacity
- Second-intention healing is not a failure: it is a regenerative strategy in implantology
- Often the best intervention in tissue augmentation is the one that facilitates natural processes instead of trying to replace them with artifices and assorted materials
The “Revolutionary” Principles (We Already Knew)
The paper identifies four key principles for success:
1. Protection from bacterial contamination → Obvious, we say it all the time
2. Phenotypic induction → Keratinized tissue must be present, even a little
3. Space maintenance → Geometry and biomechanics, fundamental
4. Flap stabilisation → Correct surgical technique
Nothing new under the sun.
Or rather, new to those who have never looked beyond the standard protocols.
The Real Value of Scientific Validation
Don’t get me wrong: studies that confirm the efficacy of techniques I have studied and applied for decades are very welcome. Scientific validation is fundamental.
But when you hold a stack of peer-reviewed publications documenting similar principles since 1998, and someone presents the same thing as “innovation” in 2024… well, let’s say historical perspective helps.
The facts speak clearly:
Our publications in the International Journal of Periodontics and Restorative Dentistry, the International Journal of Oral and Maxillofacial Implants, Heliyon, and Scientific Reports are not blog opinions: they are rigorous scientific research that anticipated by decades what is being “discovered” today.
The 2023–2025 Literature Says What We’ve Been Saying All Along
I’m not asking you to take my word for it. Let’s look at the numbers.
A network meta-analysis published in Clinical Oral Investigations in 2024 (Tommasato, Del Fabbro and colleagues) compared autogenous grafts with commercial matrices across 573 peri-implant sites. The result: to increase keratinized mucosa, vestibuloplasty with the patient’s own tissue remains the most effective technique. Collagen matrices are convenient and cause less morbidity — but they produce less keratinized tissue. A second 2024 meta-analysis in Clinical and Experimental Dental Research (Dadlani and colleagues) confirms it: xenogeneic matrices add less keratinized tissue than autogenous tissue — same aesthetics, less substance. Which is exactly the point about second-intention healing I keep making: the patient’s own biology, properly guided, can’t be bought from a catalogue.
And that keratinized tissue genuinely matters is no longer an opinion. The 2025 AO/AAP systematic review in the Journal of Periodontology (Tavelli and Barootchi), with 221 studies included, identifies a lack of keratinized mucosa as a risk factor for peri-implant recession, and an adequate band as a protective factor for margin stability. Translation: without keratinized tissue the implant recedes; with it, it holds. So where the tissue can regenerate on its own, why stop it with a membrane?
Over the long term, the 2023 review by Stefanini and Barootchi in Clinical Oral Implants Research shows that sites with soft-tissue augmentation maintain peri-implant health and stable margins in the medium to long term, while untreated implants drift apically. Guided healing — even when the wound closes by itself — is not a gamble: it is a documented strategy. And on timing, the 2025 meta-analysis by Moscowchi (Journal of Prosthodontics, 855 patients, 1,588 implants) adds a detail I’ve applied for decades: it’s better to intervene at second-stage surgery than after the prosthesis, when the keratinized-tissue gain shrinks.
Four recent reviews. None of them invented anything. They simply measured, with the rigour this topic deserved long ago.
The Future Is Already Here (since 1998, at least)
While some “discover” second-intention healing in 2024, I keep publishing cutting-edge research:
2025: “An in vitro study exploring a new method for managing peri-implant disease using the ten second technique” (Scientific Reports)
2024: “Osteotome-mediated maxillary sinus lift by localized violation and trauma below the Schneiderian membrane” (in print, with Prof. Toscano)
2023: Innovative sutures to optimise soft-tissue healing, precisely with second-intention healing in mind
2021: Five-year follow-up of flapless techniques with excellent results
The right question:
Not: “When will innovation arrive?” But: “Have you read the literature of the last 26 years?”
Conclusion: Pioneers vs Followers

Every now and then it happens: what is daily routine for me becomes “breakthrough research” for others.
And that’s fine.
I keep doing what I do best: believing in the future of regenerative dentistry built on less invasive techniques in implantology — faster, more effective — that exploit second-intention healing for keratinized-tissue augmentation.
And when, a few years from now, you read papers on regenerative techniques I’m applying today in regenerative implantology, remember this article.
❓ FAQ: Second-Intention Healing and Keratinized Tissue
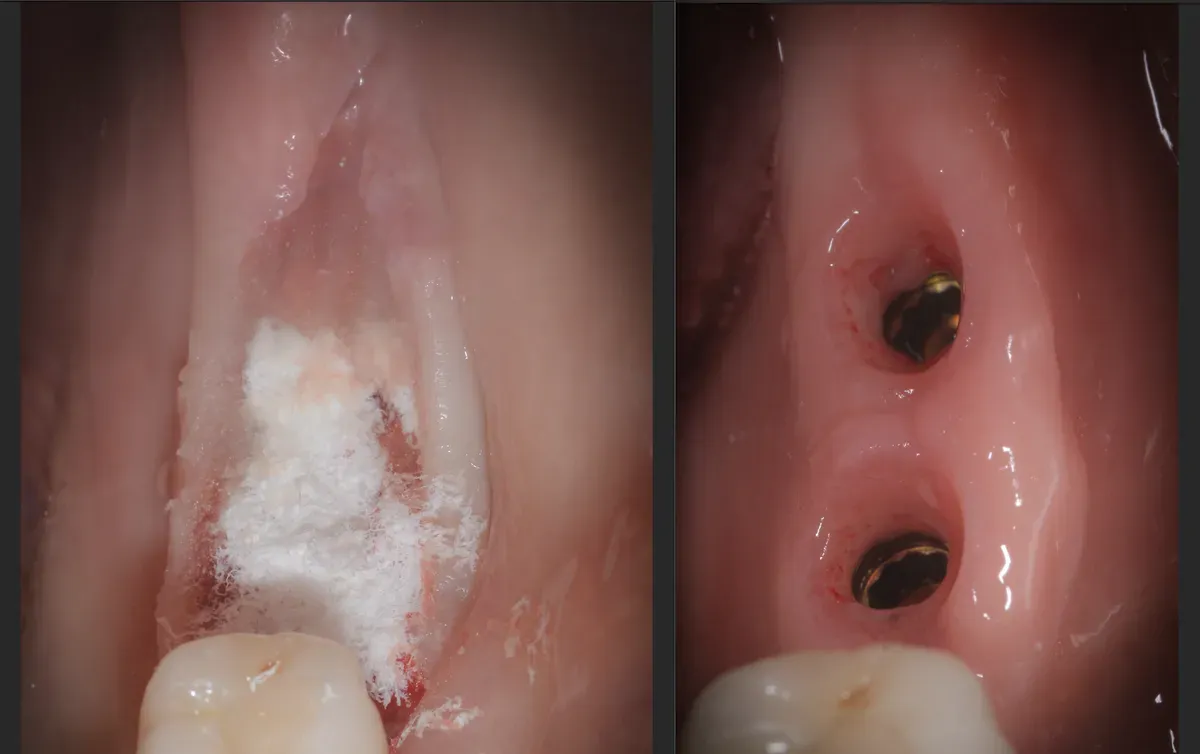
🤔 What exactly is the Gingival Open-Wound Technique?
The Gingival Open-Wound Technique increases keratinized tissue around dental implants by exploiting second-intention healing. It uses no autologous grafts or biomaterials, but the natural regenerative capacity of the tissues. We have applied it for 26 years with specific technical variations.
⏰ How long has second-intention healing actually been in use?
The principles of second-intention healing have been used for over a century. Kazanjian used them in the First World War, Tatum in the 1970s, and we have been publishing on these techniques since 1998. It is not a 2024 novelty, but a consolidated therapeutic strategy that is often misunderstood or underrated.
🛡️ Is membrane-free open healing really safe?
Absolutely yes, when well executed. It requires: protection from bacterial contamination, the presence of keratinized tissue (even minimal), space maintenance, and flap stabilisation. The 5–10-year results in our publications demonstrate excellent predictability and stability. The key is case selection and correct technique.
📚 Why was this technique held back for years?
Several factors: commercial interests (selling membranes and biomaterials), traditional academic training based on primary closure, fear of “loss of control” over the biological process, and a lack of RCT validation. The “the more complex, the better” paradigm dominated for decades, ignoring the elegance of biological simplicity.
🔬 What is the real scientific evidence since 1998?
Publications in the International Journal of Oral and Maxillofacial Implants (1998), the International Journal of Periodontics and Restorative Dentistry (1999), Scientific Reports (2025), and many others. Long-term follow-up, large case series, reproducible results. Not opinions, but peer-reviewed science in top-tier journals.
🎩 Who were the historic “pioneers” really?
Varaztad Kazanjian: Armenian-American surgeon, Harvard-trained, a pioneer of maxillofacial surgery in the First World War. Hilt Tatum: American, a “pure clinician” who devised the mini sinus lift and the split-crest in the 1970s. Both believed in second-intention healing as a treatment of choice, not a fallback.
🔎 How do you tell true innovation from “rediscovery”?
True innovation: new biological mechanisms, revolutionary instrumentation, results that were previously impossible. “Rediscovery”: restating known principles with new terminology. The 2024 Gingival Open-Wound Technique is clearly a rediscovery. Real innovation shows up in patents, not retrospective papers.
🚀 What is the future of second-intention healing?
Integration with cell therapies, targeted growth factors, tissue engineering, and personalised regenerative medicine. Second-intention healing will become increasingly “guided” but not “forced”. The future lies in biological optimisation, not in replacement with artifices. Less material, more intelligent biology.
References
- Tommasato G, Del Fabbro M, Oliva N, et al. Autogenous graft versus collagen matrices for peri-implant soft tissue augmentation. A systematic review and network meta-analysis. Clin Oral Investig. 2024. doi:10.1007/s00784-024-05684-5. PMID: 38704784.
- Dadlani S, Joseph B, Anil S. Efficacy of xenogeneic collagen matrices in augmenting peri-implant soft tissue: a systematic review and meta-analysis. Clin Exp Dent Res. 2024. doi:10.1002/cre2.937. PMID: 39104130.
- Tavelli L, Barootchi S. Prevalence, incidence, risk, and protective factors for soft tissue dehiscences at implant sites in the absence of disease: an AO/AAP systematic review and meta-regression analysis. J Periodontol. 2025. doi:10.1002/JPER.24-0119. PMID: 40489305.
- Stefanini M, Barootchi S, Sangiorgi M, et al. Do soft tissue augmentation techniques provide stable and favorable peri-implant conditions in the medium and long term? A systematic review. Clin Oral Implants Res. 2023. doi:10.1111/clr.14150. PMID: 37750532.
- Moscowchi A, Amid R, Nahvi A, et al. Timing of keratinized mucosa augmentation and peri-implant outcomes: a systematic review and meta-analysis. J Prosthodont. 2025. doi:10.1111/jopr.14064. PMID: 40302115.
Because we don’t follow trends. We create them.
P.S. If you’re a colleague and you’re thinking “this is presumptuous”, I’ll tell you “NO — and those who know me well know it, but I love the truth” and I invite you to read our publications. Then we’ll talk again. Preferably citing scientific sources.
References
Looking for a specialist?
Chirurgia Orale a Frosinone →Espansione di cresta, rialzo del seno mascellare, estrazioni complesse
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stai valutando un impianto dentale?
Ho scritto una guida in 8 capitoli che spiega tutto quello che un paziente dovrebbe sapere prima di sedersi in poltrona. Niente marketing — solo fatti, casi studio e una checklist per fare le domande giuste.
Scarica la guidaStay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment