Expansion Is Magic: Regeneration That Follows Nature
In brief — Regenerative osteo-mucosal expansion rebuilds bone and keratinized mucosa at the same time, without grafts and without sutures. The biology does the work; the surgeon only opens the door. Results that hold up after years prove this is not a fallback for difficult cases but a first-choice strategy for complex atrophy.
I want to present a case — one of many I carry out every day — that shows the power of osteo-mucosal expansion and of healing by secondary intention to achieve a complete regeneration.
And still there are those who say, from the height of their ego, that “the split crest doesn’t work” — speaking to the daughter-in-law so the mother-in-law gets the message, seasoning it all with a sarcastic little laugh.
Dear reader who recognises yourself in this character: know that it doesn’t work in your hands, which are probably both governed by the right hemisphere of your brain (and you’re not left-handed).
The humility of those always ready for new knowledge
To learn something you must “know that you do not know” (cit.). On the contrary, if you are convinced you already know everything, you will never learn anything different. In the end, you are the one who loses out.
The truth — demonstrated by hundreds of scientific papers, literature reviews, and thousands of documented cases, from Hilt Tatum onward — is that bone expansion and healing by secondary intention are not only reliable and effective: they achieve exceptional regenerative results even in the absence of grafting materials.
The question of grafting materials
Obviously, this last feature is hard to swallow for those who sell the aforementioned materials, since it hurts their sales. We Bonebenders colleagues do use biomaterials and even autologous grafts, of course — just less frequently.
And this isn’t a partisan opinion. According to PubMed, a meta-analysis in BMC Oral Health (Lin and colleagues, 2023) pooled twenty-five studies: the split crest gains on average 3.3 mm of horizontal width, and implants survive in 98.1% of cases. Numbers that stand comparison with far more invasive techniques. And when the expansion is performed without grafting materials — precisely the point that annoys those who sell them — the review by Azadi and co-workers (Oral and Maxillofacial Surgery, 2025) reports 100% implant survival and zero complications for implants placed at the same time as the expansion. Bone, left free to work, works. On why I prefer this road to traditional bone regeneration I have written at length.
Francesco’s clinical case
In the case below I used the osteo-mucosal expansion approach to regenerate the shape of the whole dental arch — not just a limited zone. The technique is essentially the same; the result is simply more striking. This is the case of Francesco, whose personal story I have already told in this post.

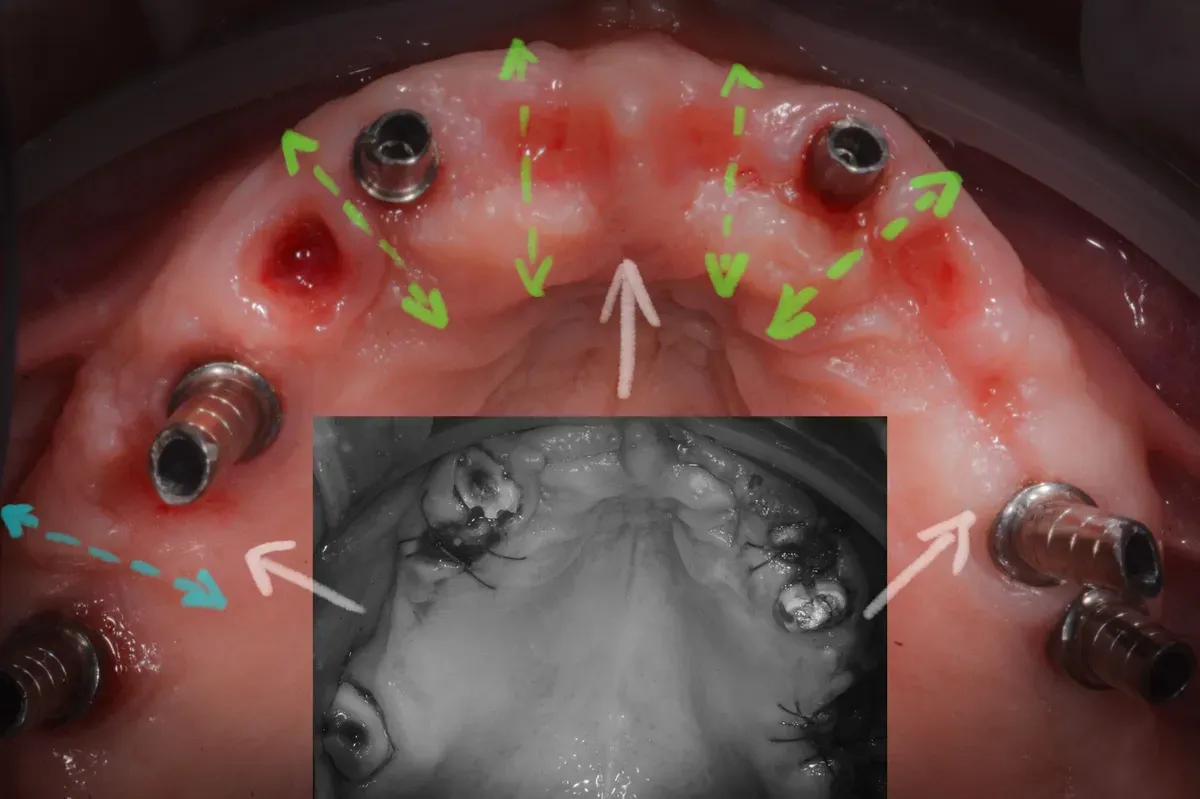
The image above is Francesco’s starting situation in the maxillary arch, after removal of an old bridge and fractured teeth.
The prognosis of the residual teeth was poor even in the medium term. Still, after discussing every possible treatment option with the patient, I chose to keep these residual teeth temporarily — to support a fixed provisional bridge and rebuild the upper arch while I carried out the regenerative procedures with expansion and placement of titanium implants.
The surgical timing
The procedures were performed in two stages: the anterior maxilla first, then the posterior maxilla.
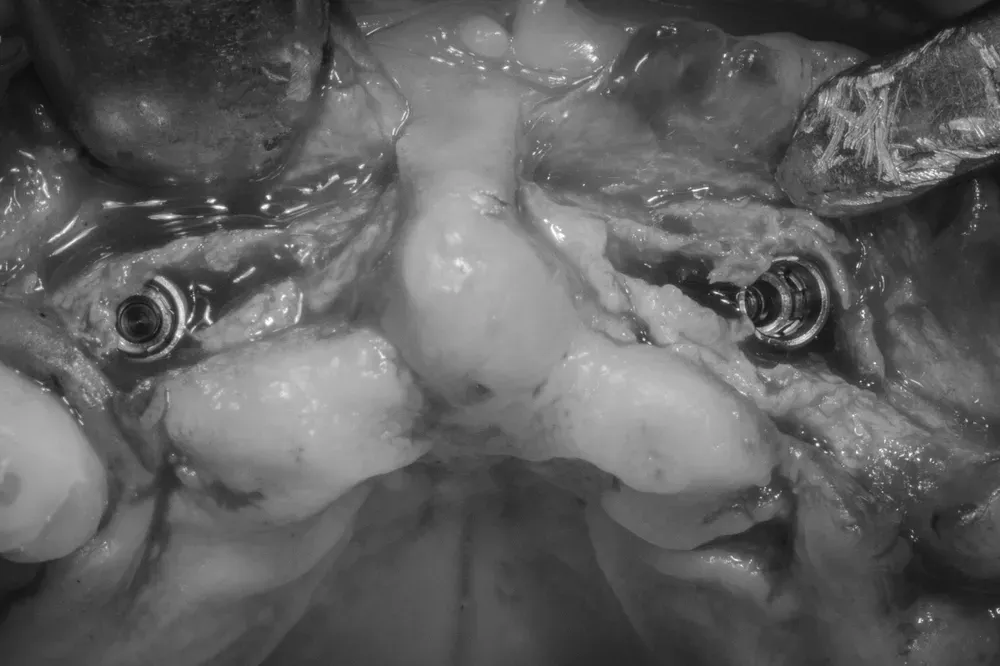
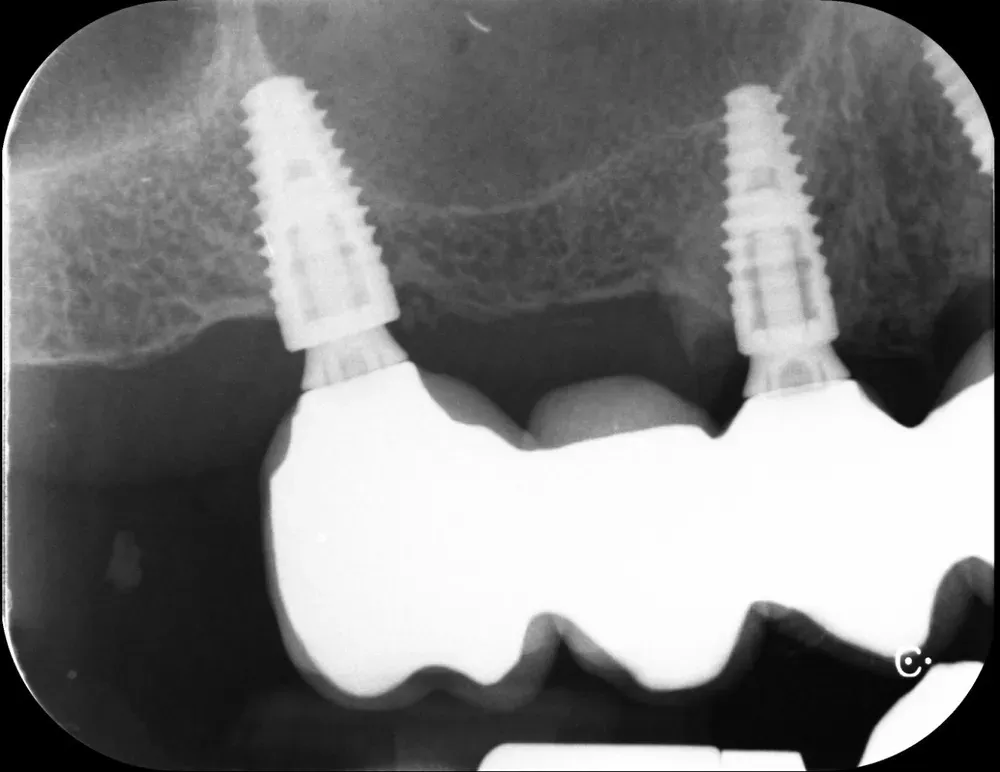
The image shows osteo-mucosal expansion with placement of two implants in the pre-maxilla, at positions 1.2 and 2.2. The space left empty will heal with the formation of new bone and keratinized mucosa.
The Cologne classification (CCARD)
The images below illustrate the pre-operative bone situation of the alveolar crest, with severe horizontal atrophy corresponding to category H3 of the Cologne Classification (CCARD).
According to the BDIZ EDI, this degree of atrophy contraindicates expansion techniques.
Personally, however, I believe that with modern instruments it is possible — and advisable — to push further, and include even this level of atrophy among the indications. This case proves it.
It is worth remembering that not all horizontal augmentation techniques deliver the same. The head-to-head comparison by Vorovenci and colleagues (Biomedical Reports, 2024) assigns guided bone regeneration a mean gain of 4.0 mm, the split crest 3.7 mm, and osseodensification 2.2 mm: GBR wins by a few tenths of a millimetre, but the split crest follows it closely — without membranes, without screws, and above all without the months of waiting. There is also a detail that often escapes notice: by condensing the trabeculae, expansion improves the implant stability quotient, as documented by the López-Valverde meta-analysis (Frontiers in Bioengineering and Biotechnology, 2025). Denser bone grips the implant better from day one — and primary stability is the real watershed between a calm rehabilitation and a gamble.
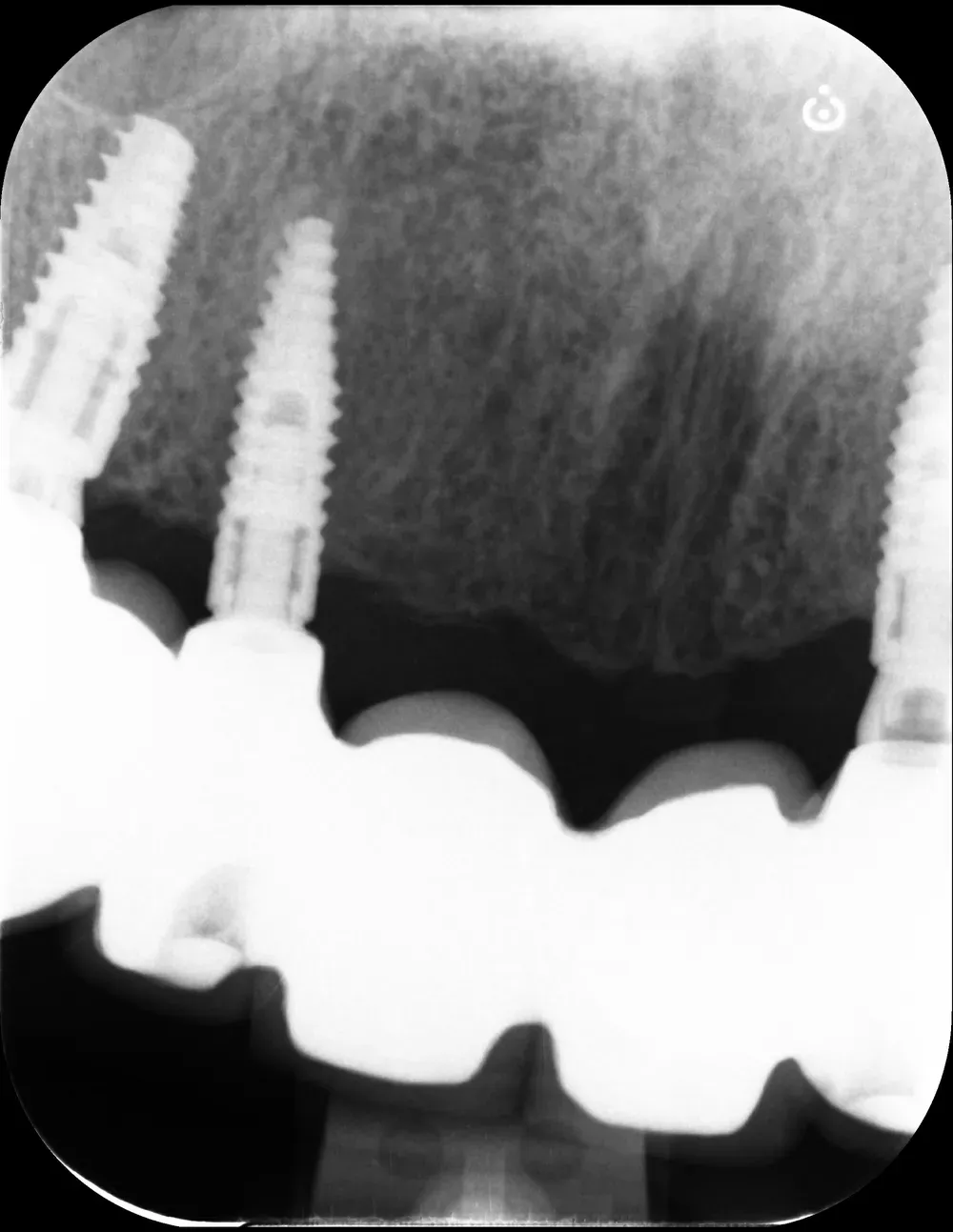
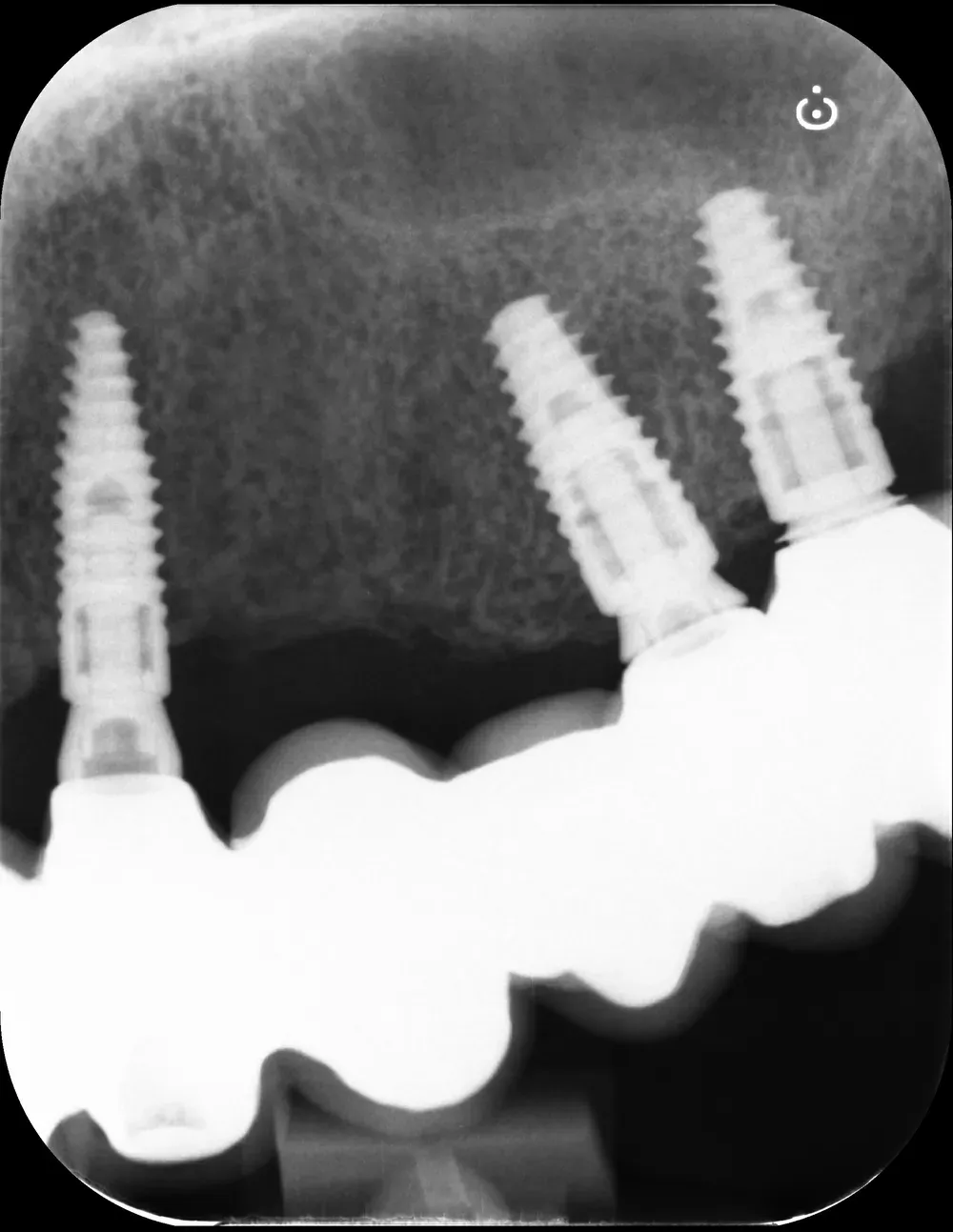
I performed this procedure under local anaesthesia and, two weeks later, treated the posterior zone. Below you can see the posterior intra-operative photos, right and left:





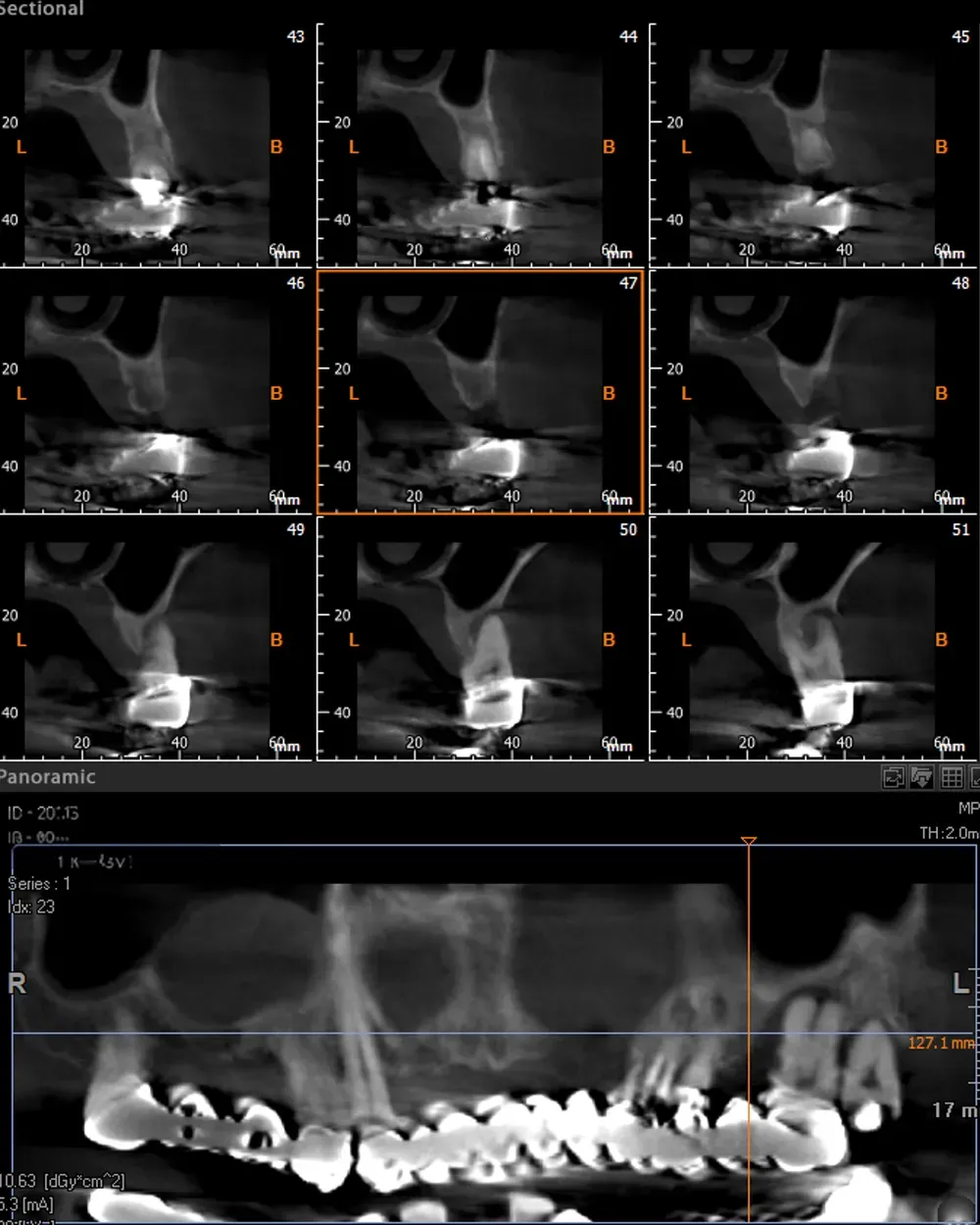
The right maxilla had category S3 CCARD atrophy at site 16 and S2 CCARD at site 14 (previously extracted), with a mucous retention cyst and an Underwood’s septum.
Implant placement with sinus lift and aspiration of the maxillary sinus mucous retention cyst
I placed two implants — at sites 16 and 14 — with a mini sinus lift and aspiration of the mucous retention cyst through a lateral access.
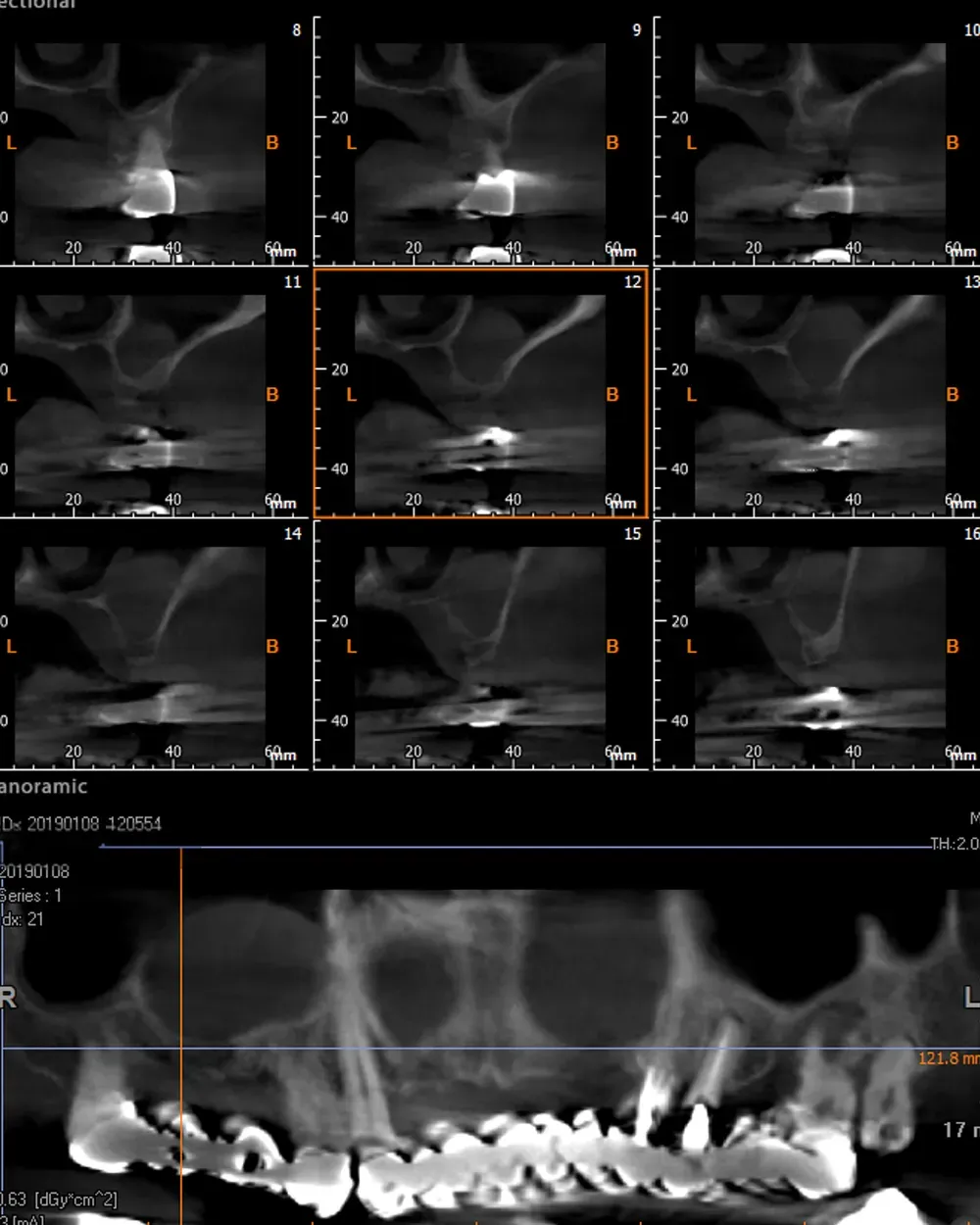
On the left side, the atrophy after tooth removal and regeneration was less severe and fell within categories S1–S2 CCARD. The next image is the CBCT of the left maxillary region before extractions.
Social life during regenerative surgical therapy
Throughout the healing phases, Francesco led a normal relational and functional life thanks to the fixed provisional prosthesis anchored to the residual teeth, which let him keep a satisfactory aesthetic appearance and face daily interactions with confidence.
Indeed, his ability to speak and eat without difficulty was crucial to his psychological and social well-being.
At the end of the surgical journey, after osseointegration of the implants, I extracted the residual teeth (not preservable in the long term) and loaded the implants with a second fixed provisional prosthesis, which continued to offer support and function.
This intermediate phase was crucial to guarantee the necessary stability while the soft tissues adapted to the new situation.
The final phase
The provisional prosthesis was then replaced by the ceramic bridge, delivering a final aesthetic and durable result that further improved Francesco’s quality of life.
The comparison between the clinical images before and after treatment (see below) is striking and leaves no room for doubt about the effectiveness of osteo-mucosal expansion techniques.

The increase in dimensions, the effect of regeneration
The two images seem to belong to two different people: the transverse dimension and the anterior alveolar crest are both markedly increased, suggesting a significant anatomical change.
What’s more, it is striking to note that all this increase was obtained without any kind of graft — which underlines the body’s natural capacity to reshape and grow in response to the surgical stimuli of healing by secondary intention.
The follow-up, years later
On the radiographic check, seven years later, the implants are in excellent health and perfectly integrated (see the images below). Francesco comes regularly for check-ups, in particular for professional hygiene sessions.

What this emblematic case demonstrates
This case demonstrates several things, among them:
- Osteo-mucosal expansion techniques are effective and reliable.
- Atrophic cases can be approached differently from the classic immediate-loading route, with a more gradual strategy — sometimes using post-extraction ridge expanders.
- Regeneration is a very valid alternative to demolitive techniques.
Do you have doubts or questions about this treatment, or about other topics on my blog? Get in touch.
References
- Lin Y, Li G, Xu T, Zhou X, Luo F. The efficacy of alveolar ridge split on implants: a systematic review and meta-analysis. BMC Oral Health. 2023;23(1):894. DOI · PubMed
- Azadi A, Hazrati P, Tizno A, Rezaei F, Akbarzadeh Baghban A, Tabrizi R. Bone expansion as a horizontal alveolar ridge augmentation technique: a systematic review and meta-analysis. Oral and Maxillofacial Surgery. 2025;29(1):32. DOI · PubMed
- Vorovenci A, Drafta S, Petre A. Horizontal ridge augmentation through ridge expansion via osseodensification, guided bone regeneration and ridge-split: systematic review and meta-analysis of clinical trials. Biomedical Reports. 2024;21(4):139. DOI · PubMed
- López-Valverde N, López-Valverde A, Blanco JA. Effectiveness of bone expansion, compacting and densification in narrow alveolar crests: a systematic review and a meta-analysis. Frontiers in Bioengineering and Biotechnology. 2025;13:1630495. DOI · PubMed

→ The technique behind this case: Crestal expansion — how it works and when to use it
References
- https://doi.org/10.1186/s12903-023-03643-2
- https://doi.org/10.1007/s10006-025-01335-5
- https://doi.org/10.3892/br.2024.1827
- https://doi.org/10.3389/fbioe.2025.1630495
- https://pubmed.ncbi.nlm.nih.gov/37986181/
- https://pubmed.ncbi.nlm.nih.gov/39808204/
- https://pubmed.ncbi.nlm.nih.gov/39161939/
- https://pubmed.ncbi.nlm.nih.gov/40635692/
Go deeper
Espansione crestale (split crest) →Allargare la cresta senza trapianto — tecnica ERE e bonebending
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stai valutando un impianto dentale?
Ho scritto una guida in 8 capitoli che spiega tutto quello che un paziente dovrebbe sapere prima di sedersi in poltrona. Niente marketing — solo fatti, casi studio e una checklist per fare le domande giuste.
Scarica la guidaStay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment