Fibrointegration: the implant that moves too much to integrate
In brief — Fibrointegration is the implant that wraps itself in fibrous scar tissue instead of bonding to bone. It can fool a radiograph; it gives way under load. It is not rejection — it is healing gone wrong. The master cause is a single one: micromotion above a critical threshold (50–150 microns) during healing, reached through inadequate primary stability, bone overheating, premature loading, or infection. It is rare and almost always preventable, because every preventive lever aims at the same target — keeping the implant still while bone grips it.
Sintesi (IT) — La fibrointegrazione è l’impianto che si circonda di tessuto fibroso cicatriziale invece di legarsi all’osso. Alla radiografia può ingannare; sotto carico cede. Non è un rigetto: è una guarigione andata storta. La causa madre è una sola — il micromovimento oltre una soglia critica (tra 50 e 150 micron) durante la guarigione — a cui si arriva per stabilità primaria insufficiente, surriscaldamento dell’osso, carico prematuro o infezione. È rara e quasi sempre prevenibile.
They tell you the same story. The implant never hurt. At three months, the radiograph looked fine. Then, the day the prosthesis is screwed on, it moves. No pus, no swelling, no sign of a war. And yet that implant is lost.
When it happens, the word that springs to mind — patient or colleague alike — is “rejection.” It is the wrong word. Implant rejection does not exist: titanium has no cells, no antigens, nothing for the immune system to attack. What happened has another name, less familiar and far more instructive: fibrointegration.
What fibrointegration is
Osseointegration is a direct bond: bone grows in contact with the titanium surface, with nothing in between, and locks it like a root. It is the discovery that changed dentistry, and Per-Ingvar Brånemark spent a lifetime proving that this — and nothing else — is what makes an implant reliable for decades.
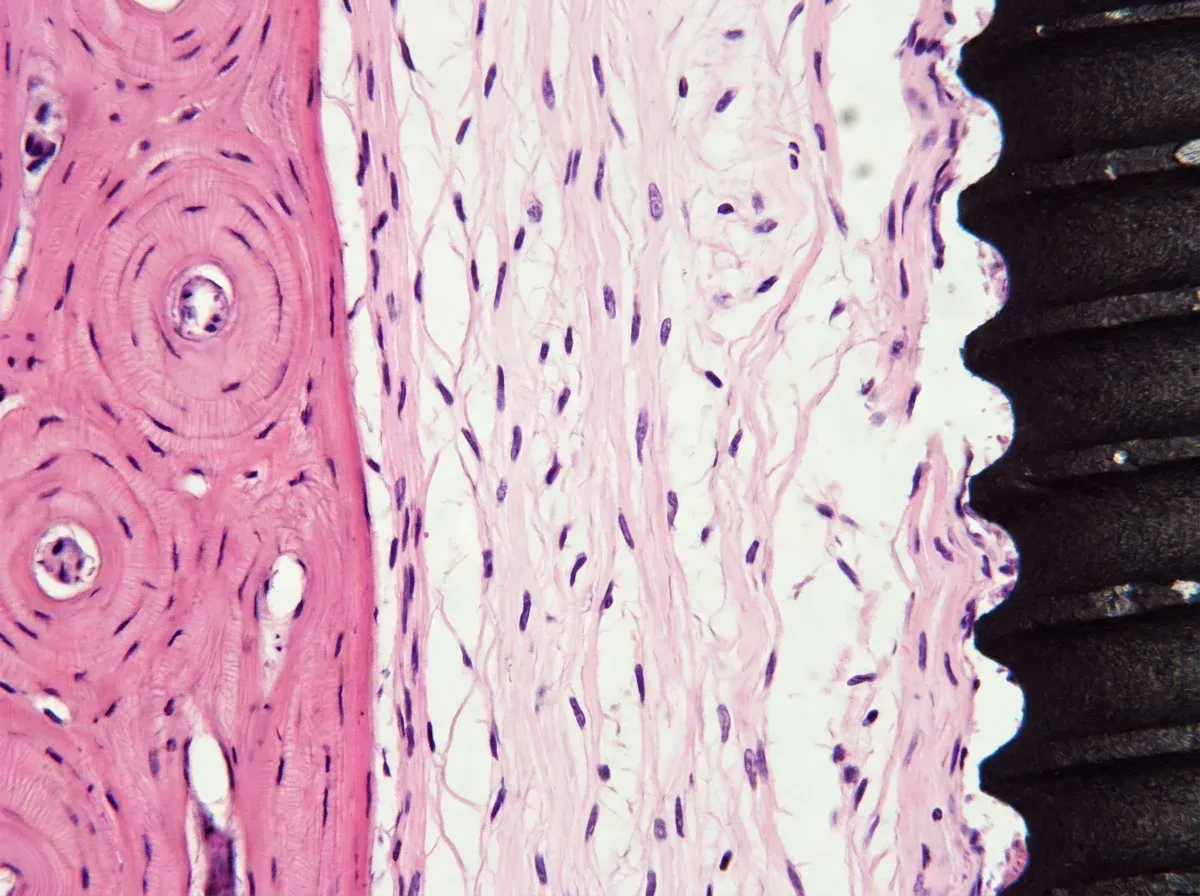
Fibrointegration is its opposite in disguise. Between implant and bone, instead of bone, a layer of fibrous connective tissue forms: a dense scar that wraps the titanium. The implant stays in place, looks integrated, sometimes even survives a careless radiograph. But that tissue is elastic, micromobile, alive in the wrong way. It can’t carry load. And when you stress it, it gives.
There was an era when fibrointegration was accepted: the blade and subperiosteal implants of the 1970s lived with a fibrous sleeve and that was considered normal. Then came the proof that bone in direct contact holds far, far better. From that point fibrointegration stopped being an outcome and became a failure.
The implant’s pseudarthrosis
There’s one image that explains it better than any diagram, and it comes from orthopaedics.
When a bone fractures, the two ends heal by knitting together — but only on one condition: that they stay still. That’s why the orthopaedist immobilises, casts, plates and screws. If the fracture keeps moving, bone can’t bridge the gap: fibrous tissue forms in its place, and a false joint is born, a pseudarthrosis. A bone that never knitted because it was never left in peace.
Fibrointegration is the implant’s pseudarthrosis. Bone bridges the titanium surface only if that surface stays still while healing does its work. Let it move too much, and instead of bone you’ll get scar. Same physics, same biology, same outcome: motion, not bad luck, decides who wins.
Hold on to this image. Everything that follows is a footnote to a single sentence: bone grips what stays still.
The master cause: micromotion
In the 1970s Brånemark required months of “stress-free” healing before an implant could be loaded, and the explanation hardened into dogma: load early and you’ll make fibrous tissue. Then someone actually went and looked at the data.
Szmukler-Moncler and colleagues reviewed the entire experimental literature on the question and found something precise, almost surprising: it isn’t early loading that builds the scar. It’s micromotion above a threshold. Below that threshold bone forms anyway, even under load. Above it, fibrosis wins. And the threshold isn’t zero, as everyone believed: it sits somewhere between 50 and 150 microns — hundredths of a millimetre (Szmukler-Moncler et al., J Biomed Mater Res, 1998; Clin Oral Implants Res, 2000).
This reversal is worth digesting. The enemy is not load. The enemy is relative movement between implant and bone during the weeks when bone is trying to grip. Everything we call a “cause of fibrointegration” — as we’ll see in a moment — is really a different road to the same place: too much motion, or dead bone that can’t heal regardless.
How direct that link is was shown, elegantly, by the work of the Helms group at Stanford. In animal models, implants placed without primary stability reproducibly develop a fibrous capsule and stay mobile: a photocopy of what we see in the clinic (Mouraret et al., J Clin Periodontol, 2014). The detail that strikes me is another one: in those implants the osteoblasts really do try — they lay down matrix, they’re active — but osteoclasts resorb the little new bone faster than it’s made. Motion tips the balance toward demolition, and the scar remains. In a second study, the same authors confirmed that an oversized osteotomy alone, leaving a gap around the implant, is enough to generate high interfacial strains, no stability, and guaranteed fibrointegration (Yin et al., J Clin Periodontol, 2016).
The causes, one by one
They are all variations on the same story. Here they are, most frequent first.
Inadequate primary stability. The first and the most common. If at placement the implant isn’t firmly gripped by bone, it micromoves with every brush of the tongue, every bite. Primary stability is friction: it comes from compression between titanium and bone. It’s missing when the osteotomy is too wide, when bone is soft (the posterior maxilla, type IV bone), when insertion torque is too low. Missing, in a word, when the implant doesn’t “bite” its bed.
Overheating and surgical trauma. Here it isn’t about motion, but about killed bone. Bone is alive, and it cooks. Eriksson and Albrektsson quantified it forty years ago, with a number that ought to be carved into every operating room: above 47 °C for one minute, bone suffers thermal damage that wrecks its ability to heal (J Prosthet Dent, 1983). A worn drill, no irrigation, excessive pressure, and you cross that threshold without noticing. Necrotic bone doesn’t integrate: it gets walled off in a fibrous repair. The good news is that with sharp instruments and copious irrigation the margin is wide — a study of 315 preparations showed that cooled rotary drills never even reached 40 °C (Aquilanti et al., J Maxillofac Oral Surg, 2022). The problem isn’t the technique. It’s the hurry.
Premature or excessive loading. Loading an implant before secondary stability — the biological kind, real bone — has replaced the mechanical kind means betting everything on the initial friction. If that friction isn’t enough to keep micromotion below threshold, you’re back to pseudarthrosis. The same holds for overload: unmanaged bruxism, a badly designed prosthesis, wrong occlusal contacts. Immediate loading is a great treatment in the wrong hands precisely for this reason: the technique is sound, but it forgives little.
Contamination and infection. A site that becomes infected during healing doesn’t lay down bone: it defends itself. It is one of the classic causes of early loss, alongside surgical trauma and premature loading, in Esposito and colleagues’ large review of the etiopathogenesis of implant failures (Eur J Oral Sci, 1998). Hence the weight of asepsis and of antibiotic cover when it is genuinely indicated.
Unfavourable surface and geometry. All else being equal, the shape and the skin of the implant change who wins the race for the surface. This is the theme of myofibroblasts versus osteoblasts: macro- and microgeometry and the surface treatment steer cells toward the bone lineage or the fibrous one. Modern surfaces — rough, hydrophilic — give osteoblasts an enormous head start. If you’re still in love with smooth implants, that’s the detail to reflect on.
The biological terrain. Above all of it sits the patient. Poorly vascularised bone, smoking, badly controlled diabetes, certain chronic therapies all lower the capacity to heal — and with it the threshold of tolerated micromotion. I won’t relitigate them here because they deserve an article of their own: I lined them up when I explained why implant failure is rare but worth understanding.
How to prevent it
Fibrointegration isn’t treated: it’s prevented. That’s a hard point to accept, but it’s honest to say. Once the fibrous capsule has formed, the clinical options almost always shrink to one — remove the implant and start over (Yin et al., 2016). All the value sits upstream. And since the cause is a single one, prevention has a single target too: give bone the stillness it needs to grip, on bone that is alive. Here are the concrete levers.
Build real primary stability. That means fitting the osteotomy to the bone, not the other way round: under-preparing in soft bone, choosing geometry and compression for the site instead of chasing one universal protocol. Techniques that condense bone rather than remove it — osseodensification, and in our world the expansion techniques — go in exactly this direction: they densify the bed, raise friction, cut micromotion at the root. More grip, less motion, less fibrosis.
Measure stability, without fetishising the number. Insertion torque and resonance frequency analysis (ISQ) help you judge whether your anchorage is good. But read them for what they are. A recent meta-analysis of 48 studies found that ISQ and torque correlate only moderately, and that the ISQ value at placement does not on its own predict implant survival (Tisci et al., Clin Implant Dent Relat Res, 2026). Translation: they’re warning lights, not oracles. The number informs you; it doesn’t decide for you. Clinical judgement stays sovereign.
Operate on cold bone. Sharp drills, replaced as they wear; graded preparation; copious irrigation; controlled speed and pressure. It all serves one thing — staying below 47 °C — and protecting the clot that, in the first minutes on titanium, launches contact osteogenesis. Bone that dies doesn’t integrate.
Match the load to the stability. Immediate loading when primary stability is high enough to keep micromotion below threshold; otherwise wait, with no romanticism. Splint implants to spread the forces, design a gentle occlusion, intercept bruxism. It isn’t a matter of courage: it’s a matter of numbers.
Cleanliness and selection. Aseptic field, periodontitis treated before — not after — antibiotic prophylaxis when indicated. And don’t operate on a biological terrain you could improve first: quitting smoking, controlling blood sugar. Often the most important decision is the decision to wait.
When it happens anyway
I’d be dishonest if I closed by saying that, with all of this done, fibrointegration disappears. Rarely, but it can happen even to the textbook-perfect implant. A terrain that heals badly without your knowing, a parafunction nobody intercepted, an individual tolerance threshold lower than expected. It is a rare event — with today’s surfaces, marginal compared with late infection and peri-implantitis — but real.
And there’s a frontier worth watching with cautious curiosity. The very experiments that proved the link between missing stability and fibrosis also showed that, by amplifying certain biological signals (the Wnt pathway), a fibrous interface can be pushed to lay down bone. In the lab. In mice. Not in my office, not today, not on your implant. For now the rule holds, as ever: prevent first, because afterward you remove.
The implant doesn’t choose to fail. We are the ones who decide whether to grant bone the stillness it needs to grip it. That’s all there is to it — and it isn’t little.
Frequently asked questions
Is fibrointegration the same as rejection? No. Rejection is an immune reaction against transplanted living tissue, and titanium is not living tissue. Fibrointegration is a mechanical healing problem: disturbed by too much motion or by surgical trauma, bone repairs with fibrous scar tissue instead of bone. The implant is not attacked — it simply does not integrate.
How do I know if an implant is fibrointegrated? Early on, often you can’t. The implant doesn’t hurt and the radiograph can look calm. The problem shows up when you load it with the prosthesis: it moves, it can’t take chewing forces. That’s why fibrointegration is prevented, not diagnosed in time.
Can a fibrointegrated implant be treated, or must it be removed? Today, in practice, it has to be removed: once the fibrous capsule has formed, you can’t talk bone into replacing it. There is laboratory research trying to reawaken bone formation even in these cases, but it is far from the clinic. The real treatment is still prevention.
Does immediate loading cause fibrointegration? No, not by itself. What builds fibrous tissue is not loading as such, but excessive micromotion during healing. If primary stability is high and micromotion stays below threshold, immediate loading is an excellent technique. It becomes dangerous when that stability is missing.
If primary stability is enough, why do textbook-perfect implants still fail? Because the threshold of tolerated motion isn’t the same for everyone. Poorly vascularised bone, a smoker, badly controlled diabetes, unrecognised bruxism all lower that threshold: the same micromotion healthy bone ignores, fragile bone turns into fibrosis. Stability is necessary, not always sufficient.
How common is fibrointegration? It’s rare. With modern implant surfaces and disciplined surgical technique it is a marginal event compared with the other causes of failure. But it exists, and it is almost always preventable — which is exactly why it’s worth knowing.
References
- Szmukler-Moncler S, Salama H, Reingewirtz Y, Dubruille JH. Timing of loading and effect of micromotion on bone-dental implant interface: review of experimental literature. J Biomed Mater Res. 1998;43(2):192-203. DOI · PMID: 9619438
- Szmukler-Moncler S, Piattelli A, Favero GA, Dubruille JH. Considerations preliminary to the application of early and immediate loading protocols in dental implantology. Clin Oral Implants Res. 2000;11(1):12-25. DOI · PMID: 11168189
- Mouraret S, Hunter DJ, Bardet C, Popelut A, Brunski JB, Chaussain C, et al. Improving oral implant osseointegration in a murine model via Wnt signal amplification. J Clin Periodontol. 2014;41(2):172-180. DOI · PMID: 24164629
- Yin X, Li J, Chen T, Mouraret S, Dhamdhere G, Brunski JB, et al. Rescuing failed oral implants via Wnt activation. J Clin Periodontol. 2016;43(2):180-192. DOI · PMID: 26718012
- Eriksson AR, Albrektsson T. Temperature threshold levels for heat-induced bone tissue injury: a vital-microscopic study in the rabbit. J Prosthet Dent. 1983;50(1):101-107. DOI · PMID: 6576145
- Esposito M, Hirsch JM, Lekholm U, Thomsen P. Biological factors contributing to failures of osseointegrated oral implants. (II). Etiopathogenesis. Eur J Oral Sci. 1998;106(3):721-764. DOI · PMID: 9672097
- Aquilanti L, Antognoli L, Rappelli G, Di Felice R, Scalise L. Heat generation during initial osteotomy for implant site preparation: an in vitro measurement study. J Maxillofac Oral Surg. 2022;22(2):313-320. DOI · PMID: 37122802
- Tisci A, Fanelli F, Caponio VCA, Zhurakivska K, Dioguardi M, Troiano G. Resonance frequency analysis and clinical outcomes in implant dentistry: a systematic review and meta-analysis. Clin Implant Dent Relat Res. 2026;28(3):e70156. DOI · PMID: 42117690
FAQ
- Is fibrointegration the same as rejection?
- No. Rejection is an immune reaction against transplanted living tissue, and titanium is not living tissue. Fibrointegration is a mechanical healing problem: disturbed by too much motion or by surgical trauma, bone repairs with fibrous scar tissue instead of bone. The implant is not attacked — it simply does not integrate.
- How do I know if an implant is fibrointegrated?
- Early on, often you can't. The implant doesn't hurt and the radiograph can look calm. The problem shows up when you load it with the prosthesis: it moves, it can't take chewing forces. That's why fibrointegration is prevented, not diagnosed in time.
- Can a fibrointegrated implant be treated, or must it be removed?
- Today, in practice, it has to be removed: once the fibrous capsule has formed, you can't talk bone into replacing it. There is laboratory research trying to reawaken bone formation even in these cases, but it is far from the clinic. The real treatment is still prevention.
- Does immediate loading cause fibrointegration?
- No, not by itself. What builds fibrous tissue is not loading as such, but excessive micromotion during healing. If primary stability is high and micromotion stays below threshold, immediate loading is an excellent technique. It becomes dangerous when that stability is missing.
- If primary stability is enough, why do textbook-perfect implants still fail?
- Because the threshold of tolerated motion isn't the same for everyone. Poorly vascularised bone, a smoker, badly controlled diabetes, unrecognised bruxism all lower that threshold: the same micromotion healthy bone ignores, fragile bone turns into fibrosis. Stability is necessary, not always sufficient.
- How common is fibrointegration?
- It's rare. With modern implant surfaces and disciplined surgical technique it is a marginal event compared with the other causes of failure. But it exists, and it is almost always preventable — which is exactly why it's worth knowing.
References
- https://doi.org/10.1002/(sici)1097-4636(199822)43:2%3C192::aid-jbm14%3E3.0.co;2-k
- https://doi.org/10.1034/j.1600-0501.2000.011001012.x
- https://doi.org/10.1111/jcpe.12187
- https://doi.org/10.1111/jcpe.12503
- https://doi.org/10.1016/0022-3913(83)90174-9
- https://doi.org/10.1046/j.0909-8836..t01-6-.x
- https://doi.org/10.1007/s12663-022-01800-8
- https://doi.org/10.1111/cid.70156
Looking for a specialist?
Implantologia a Frosinone →Impianti dentali, carico immediato e rigenerazione ossea
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stai valutando un impianto dentale?
Ho scritto una guida in 8 capitoli che spiega tutto quello che un paziente dovrebbe sapere prima di sedersi in poltrona. Niente marketing — solo fatti, casi studio e una checklist per fare le domande giuste.
Scarica la guidaStay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment