Immediate Loading: Technique, Benefits and When It's Indicated
In brief — Immediate-load implantology restores aesthetics and function within 24-48 hours of implant placement. It requires adequate primary stability and good bone quality. It is not suitable for every case: delayed loading remains indicated with compromised bone or significant risk factors.
Sintesi (IT) — L’implantologia a carico immediato ripristina estetica e funzione entro 24-48 ore dall’inserimento implantare. Richiede stabilità primaria adeguata e buona qualità ossea. Non adatta a tutti i casi: il carico differito resta indicato con osso compromesso o fattori di rischio significativi.
Losing one or more teeth can compromise not only the smile, but the ability to chew properly, speak with confidence and relate to others without embarrassment.
Immediate-loading implantology is nothing new. In Italy, a few pioneers were already doing it back in the 1960s…
It is a solution that restores the mouth’s function right after placing one or more implants (not necessarily the whole mouth!).
But is it really right for everyone? When can it be applied, and what are the real benefits over conventional techniques?
In this article I will go through every aspect of the technique — how it works, what the correct indications are, and when delayed loading is the wiser option instead.
As a surgeon devoted to what I call custom regeneration, I believe every treatment must be tailored to the patient, weighing anatomy and clinical conditions one case at a time.
What Immediate-Loading Implantology Is
Immediate-loading implantology is a surgical technique that replaces lost teeth with titanium implants, which act as new artificial roots.
The procedure aims to restore not only the smile, but functional well-being and everyday quality of life.
Its defining feature is the immediate placement of a temporary prosthesis on the freshly inserted implants, letting the patient smile and chew (with due care) within hours of surgery. In cases of total edentulism of one or both arches, the technique can give the mouth back its full function in remarkably little time.
Immediate loading is now widely used in clinical practice. Yet it is sometimes proposed even when it is not strictly necessary, occasionally leading to the unjustified removal of teeth that could have been saved.
For this reason it is essential to turn to qualified professionals who assess each case with care and honesty.
How the Technique Works
Biologically, the procedure replaces the tooth root with a titanium implant and applies a temporary prosthesis straight away.
This prosthesis restores aesthetics immediately and allows a normal social life during healing. In the early phase, soft foods can be chewed with care, gradually moving to firmer foods after the first month.
It is a biological process similar to the healing of a long-bone fracture.
This approach allows provisional rehabilitation of a single tooth, an entire arch or the whole mouth within 24 hours.
The temporary prosthesis has both aesthetic and functional roles, but it must be managed carefully in the first weeks to secure the success of osteointegration.

Custom Regeneration and Immediate Loading
Does immediate loading belong to the philosophy of custom regeneration? The answer is nuanced: yes and no.
They can be compatible, even simultaneous — or opposed, depending on the clinical circumstances. What stays essential is that the therapy is tailored to the patient, and that at least the treatment plan is personalised, even without guided tissue regeneration.
Not every treatment suits every patient, and not every patient suits every treatment.
Individual assessment is the foundation of every therapeutic success.
Immediate vs Delayed Loading: The Differences
Dentistry distinguishes two main implant approaches: immediate loading and delayed loading.
The fundamental difference lies in the timing of the prosthesis after implant placement.
In immediate loading, the temporary prosthesis is applied within 24-48 hours of insertion.
In delayed loading, complete osteointegration (usually 2-4 months) is awaited before loading the implants.
Both have their own indications, and neither is superior in absolute terms: the choice depends entirely on the clinical case.
When Immediate Loading Is Indicated
Generally, immediate loading is reserved for cases where the implants’ primary stability after insertion is sufficient to withstand the mechanical stresses of the first three weeks of healing — the most critical period.
That stability is sought in the densest areas of the maxillary or mandibular bone, especially at the implant apex, where it is possible to achieve cortical anchorage (in the densest, most stable part of the bone).
The literature confirms this without hedging. A systematic review and meta-analysis by Hamilton and colleagues (Clinical Oral Implants Research, 2023), which sifted through 68 studies on immediate placement and loading of the single tooth in the maxillary aesthetic zone, reports high survival rates — but only where patient- and site-selection criteria were strict. It is not the technique that decides the outcome: it is the primary stability at the moment of insertion, and the discipline with which you choose who to operate on and who not.
Dental implants are not simple “screws”, even if they may look like it.
Although they have self-tapping threads and a cylindrical or conical shape, the initial stability generated by screwing into bone must be progressively replaced by a new stability arising from the growth of new bone onto the implant surface within the first month. This process, called osteointegration, is the basis of long-term success.
If the implant material were not osteointegrable, it would inevitably be rejected by the body.
To picture it: a carpenter’s screw driven into bone would fall out after two weeks, because it lacks the surface features that allow bone-cell adhesion and growth.
When Delayed Loading Is Preferable
When bone density and anatomy do not allow adequate primary stability, or when the site is non-aesthetic and the patient can wait without discomfort, it is preferable to await complete bone healing (3-4 months) before placing an implant-anchored prosthesis.
Sometimes removable provisionals or temporary solutions ensure a normal life during healing.
Personally, I have never left a patient without teeth. It is simply not part of how I work.
The most suitable approach is dictated by the specific clinical conditions, carefully weighing the state of bone and gingival structures alongside the patient’s general health.
The Stages of Immediate-Loading Surgery
Immediate-loading surgery unfolds through several well-planned stages.
The first is a thorough examination: a complete medical history is taken and the patient’s expectations are assessed.
A series of specialist diagnostic exams follows, such as panoramic radiography and Cone Beam CT, essential to gauge the quantity and quality of available bone precisely. Laboratory tests are often needed too, and sometimes further specialist visits.
Next, digital impressions or intraoral scans of the arches are acquired, so the dental laboratory can prepare the temporary prosthesis even before surgery.
Instrumental exams allow us to simulate, before surgery, the three-dimensional position of the implants to make sure they will not interfere with noble anatomical structures such as the inferior alveolar nerve, the maxillary sinus or the roots of adjacent teeth that must be preserved.
Personalising the Treatment Plan
Personally, I love choosing the number and dimensions of the implants according to each patient’s anatomy, rather than relying on rigid, standardised protocols. Always in the spirit of custom regeneration, I believe every case deserves individual study to optimise the final result.
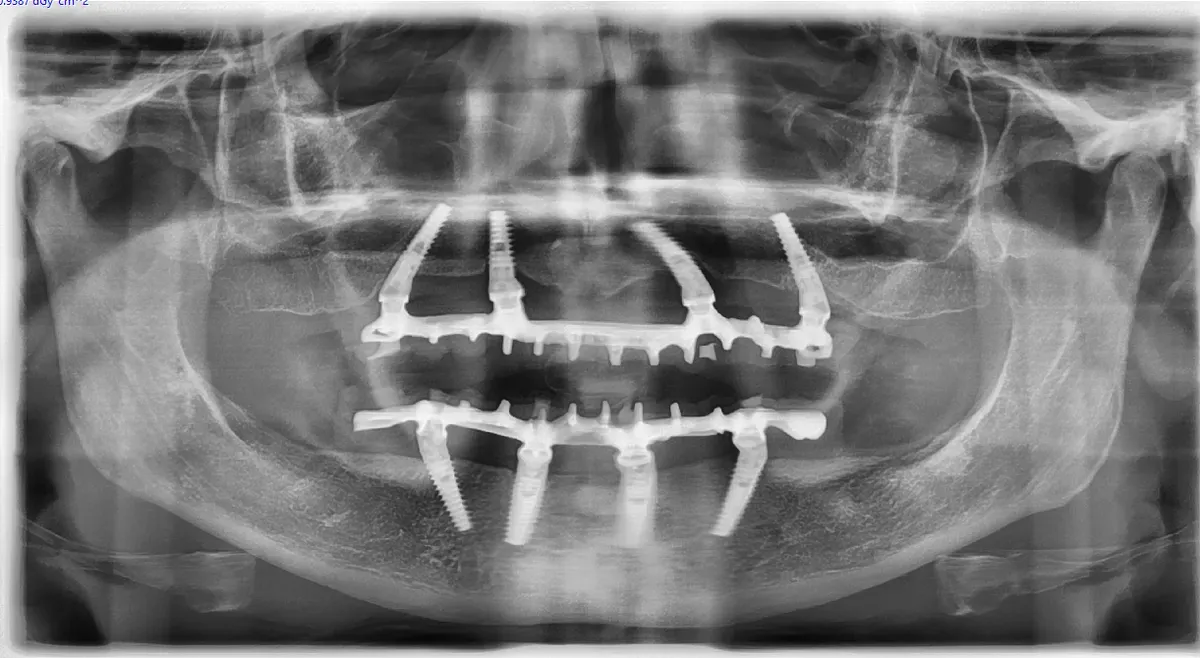
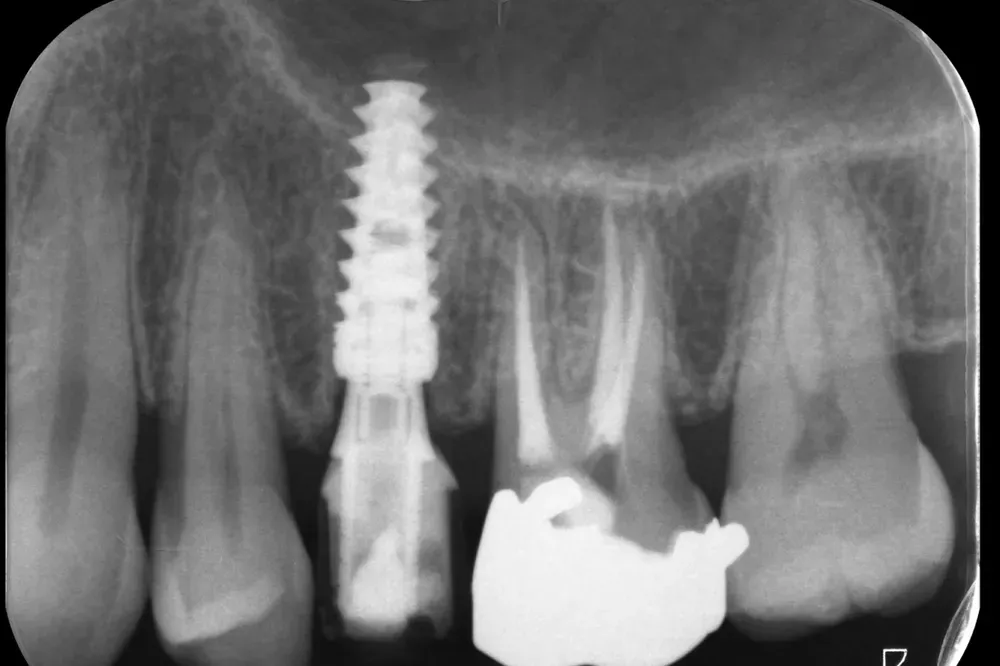
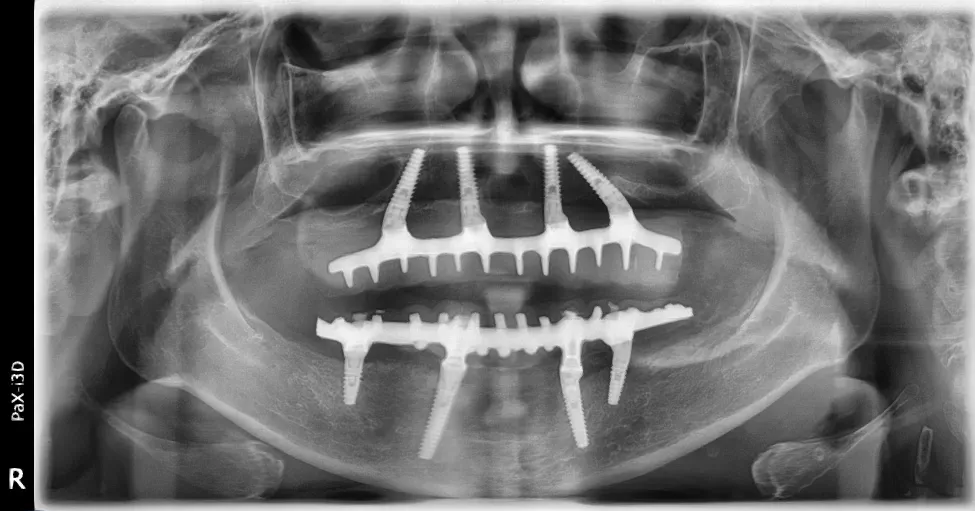
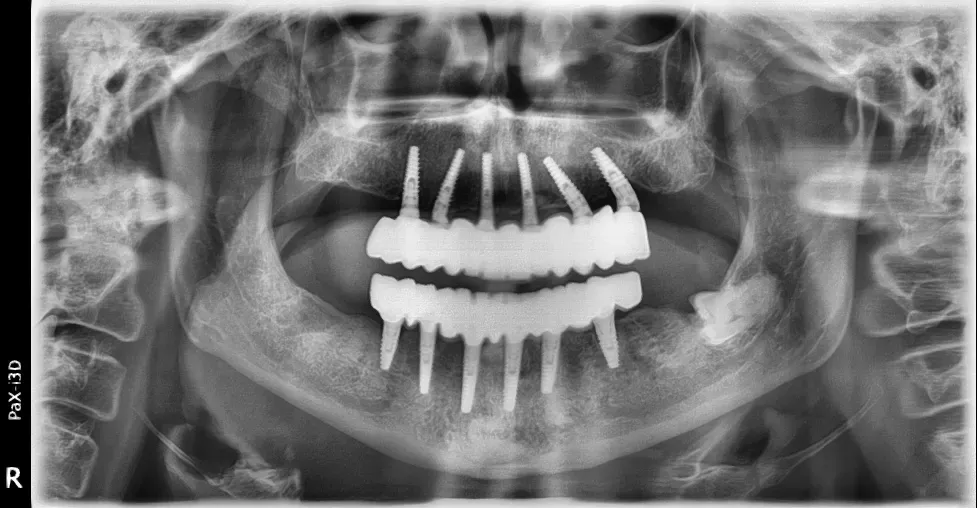
The radiographs that follow bear witness to some of the many technical solutions I have used for immediately loaded arches over my career. Every case brings different challenges and demands a personalised approach.

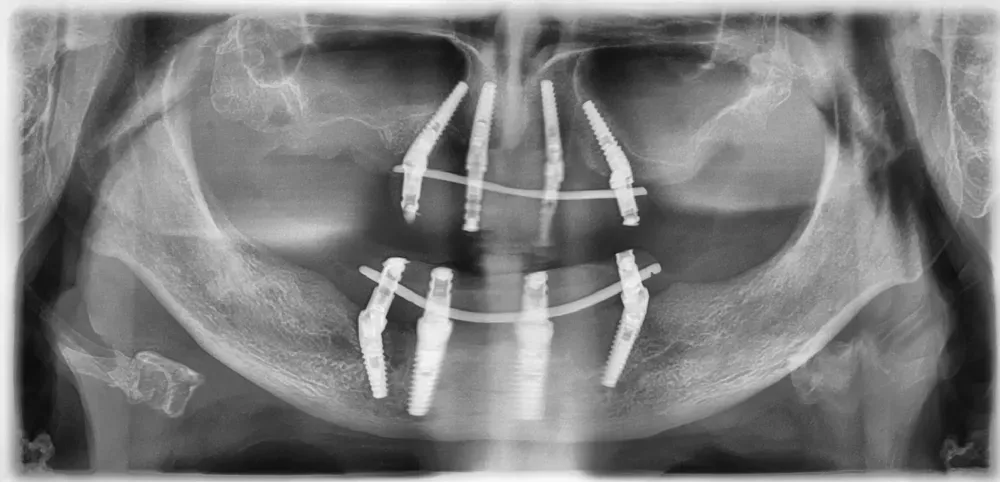
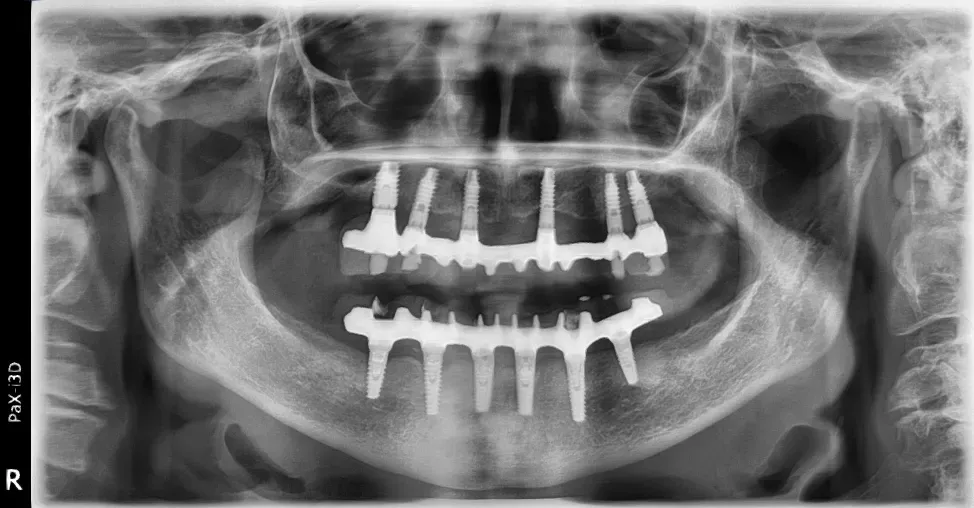
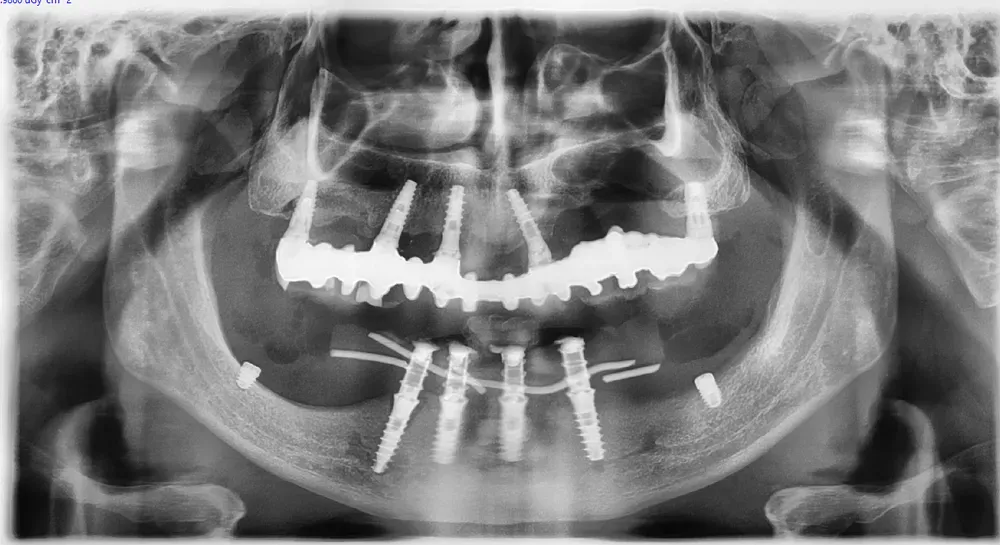
Even in elderly patients with removable dentures and critical bone conditions, immediate-loading surgery can be carried through successfully. This is also where the choice plays out between a standardised full-arch rehabilitation and a biological approach tailored to the patient: I have written about it in custom regeneration versus All-on-X.
It all depends on general health and residual anatomy. There is no absolute age limit, only a careful weighing of the risk-benefit ratio for each patient.
Benefits of Immediate-Loading Implantology
Immediate loading offers several advantages over conventional delayed-loading techniques, when applied in appropriate cases.
The most obvious benefit, and the one patients value most, is the chance to smile and socialise normally just hours after surgery — no months of waiting with removable provisionals, no visible gaps.
Psychologically, the impact is considerable. Many patients report an immediate lift in self-esteem and social life, able to attend important events, work meetings or simply go out for dinner without the embarrassment of missing teeth or unstable removable prostheses.
But there is more than a psychological benefit. When the temporary prosthesis is placed at once, the soft tissues around the implant also tend to hold up better: the meta-analysis by Qin and colleagues (International Journal of Oral & Maxillofacial Implants, 2023), across eight randomised trials in the aesthetic zone, measured nearly half a millimetre less buccal mucosal recession compared with delayed loading, with no difference in implant survival. And time does not contradict the finding. A ten-year randomised trial by Donker and colleagues (Journal of Clinical Periodontology, 2024) reports 100% implant survival at ten years, with marginal bone loss comparable between immediate and delayed provisionalisation. In the right cases, immediate loading is not a compromise: it is the choice that best protects the architecture of the tissues.
Another significant advantage is the reduced total number of surgeries. In the conventional delayed technique, two separate operations are often needed: one to place the implants and one later to connect the prosthetic abutments.
With immediate loading, when possible, everything is done in a single surgical session, reducing patient stress and overall biological healing times.
Functionally, the ability to gradually chew soft foods from the first weeks helps maintain some stimulation of bone tissue, which according to some studies may favour osteointegration through controlled mechanical loading.
Naturally, this must happen with care and by strictly following the surgeon’s instructions, to avoid harmful overload.
Nor should the indirect economic side be overlooked: fewer appointments and fewer surgeries mean fewer days off work and lower travel and lost-time costs. For many patients, that is no small factor in choosing treatment.
Contraindications and Risk Factors
In general, immediate-loading implantology has no absolute contraindications that entirely prevent its use.
However, several risk factors must be carefully monitored and assessed to secure success and minimise complications.
It would be dishonest to tell only the bright side of the story. Not every clinical context rewards the immediate approach. A meta-analysis by Wang and colleagues (Acta Odontologica Scandinavica, 2024), across sixteen randomised trials and almost 1,600 implants supporting removable prostheses, found slightly lower survival and greater marginal bone loss with immediate loading compared with conventional loading. Small differences, but real. The lesson is always the same: where bone is rarefied — or there is genuinely too little of it — forcing the timing has a price, and delayed loading becomes the wiser choice again.
Systemic and circulatory diseases are a first area of attention. Patients with severe heart disease, uncompensated coagulation disorders or severe peripheral vascular disease require multidisciplinary assessment before proceeding. Bone quality plays a crucial role: patients with advanced osteoporosis or prior head-and-neck irradiation may present qualitatively compromised bone.
Diabetes mellitus deserves a separate note. Diabetic patients with circulatory complications and uncontrolled blood-sugar levels must bring glycaemia back within normal parameters before surgery, exactly as for any other surgical procedure. Well-controlled diabetes, with glycated haemoglobin below 7%, is not a contraindication to immediate loading.
Cigarette smoking is one of the most relevant risk factors in modern implantology. Nicotine and the other components of tobacco smoke reduce tissue vascularisation, impair the local immune response and delay bone healing. In heavy smokers (more than 10 cigarettes a day), the failure rate of immediately loaded implants can rise significantly.
Some drug therapies call for particular attention.
Bisphosphonates, used to treat osteoporosis and some oncological conditions, can increase the risk of jaw osteonecrosis after invasive surgery. Patient age, by contrast, does not significantly affect the feasibility of immediately loaded implants.
Possible Risks and Complications
Placing dental implants is a genuine surgical procedure, not a routine technical act. As such, it carries risks that must be known and discussed with the patient during informed consent.
The most common risks in conventional implantology include post-operative pain, swelling, bruising, inflammation and infection. In most cases these adverse events are mild and resolve spontaneously or with appropriate medical therapy within a few days. Paraesthesia — altered sensation such as tingling or hypoaesthesia — can occur when an implant comes very close to the inferior alveolar nerve or other peripheral nerves during insertion.
One point worth clarifying concerns the so-called “rejection” of implants. For both immediate and delayed-loading implants, the risk of true rejection due to material incompatibility is practically nil.
Implants are made of medical-grade pure titanium, or ceramic (zirconia) for those who prefer it, both highly biocompatible materials.
In centres of excellence, only pure, sterile, decontaminated titanium is used, with certified European manufacturing. It is crucial to use implants recognised by the Italian Ministry of Health and bearing the European CE mark. Implants of dubious origin can cause severe inflammatory reactions due to poor sterilisation, contamination by industrial processing residues or low-quality metal alloys.
What is commonly called “rejection” is in reality only a failed osteointegration. With markedly reduced bone structure, even after grafts or bone expansions, there is a slight increase in the risk of failed integration.
Statistically, that risk is a tiny percentage (generally below 2% in healthy non-smokers), and in these cases so-called “fibrointegration” occurs.
A fibrointegrated implant, though free of active infection, is slightly mobile because it is stabilised by fibrous connective tissue rather than bone. This condition makes the implant unusable and requires its removal and replacement with a new implant, generally slightly larger.
The Fixed Prosthesis in Immediate Loading
The fixed prosthesis plays a fundamental role in the overall success of immediate-loading treatment. After any extraction of compromised residual teeth — where the clinician deems it necessary and appropriate after careful assessment — the implants are placed and the temporary prosthesis is applied immediately. When a tooth must be lost anyway, the implant placed in the same socket is often the best route: I have explained why in immediate implant placement is (almost) always the best solution.
This provisional device is made before surgery from the impressions or digital scans, and is personalised on the day of surgery to fit the new anatomy perfectly. The temporary prosthesis is generally made of reinforced acrylic resin, a light material that reduces the load on the implants during the critical healing phase.
From the delivery of the temporary prosthesis to the definitive fixed one, immediate loading involves a relatively short interval, generally 3 to 4 months. During this time the patient faces no significant limitations: soft foods for the first three weeks, then a gradual return to firmer foods, speaking normally and socialising without embarrassment.
The primary goal of every immediate-loading procedure is complete osteointegration, a fascinating biological process in which the new titanium roots must be accepted by the body and gradually integrated into the surrounding bone and gingival tissue.
After the final fixed prosthesis is placed, scrupulous, constant oral hygiene and periodic check-ups are essential.
A well-integrated implant, in a patient who keeps optimal oral hygiene and attends regular follow-ups, has no predefined time limit.
Barring particular changes in general health, it can last a lifetime, offering a durable, functional smile — and that is no figure of speech: twenty-year survival studies document it. With the right care and preventive attention, complications such as peri-implantitis, an inflammatory disease affecting the tissues around implants, can be prevented.
Frequently Asked Questions on Immediate-Loading Implantology
How long does an immediately loaded implant last?
An immediately loaded dental implant, once properly integrated and maintained with good oral hygiene, can last a patient’s lifetime. The literature reports survival rates above 95% at 10 years for immediately loaded implants in healthy patients. Longevity depends mainly on general health, home and professional hygiene, control of risk factors such as smoking, and regular follow-up visits.
Can I eat right after immediate-loading surgery?
Yes, but with important precautions. In the first 24 hours it is best to stick to cold or room-temperature foods that are soft and require no chewing, such as ice cream, yoghurt, smoothies and purees. From 24 hours up to about three weeks, you can chew soft foods carefully while avoiding the operated area. After the first month, when osteointegration is well advanced, a normal diet can be gradually resumed.
What is the main difference between immediate and delayed loading?
The key difference lies in the timing of the prosthesis. In immediate loading, the temporary prosthesis is placed within 24-48 hours of implant insertion, giving the patient immediate aesthetic and functional recovery. In delayed loading, complete osteointegration (3-4 months) is awaited before loading the implants. The choice depends on the primary stability achieved at insertion and the patient’s anatomy.
When is immediate loading not possible?
Immediate loading is not indicated when adequate primary stability cannot be achieved at implant insertion. This typically happens with low-density bone, after recent bone grafts not yet consolidated, in patients with severe uncontrolled bruxism, in heavy smokers unwilling to quit, in decompensated diabetics or in the presence of active infection at the site.
Is immediate loading painful?
Immediate-loading surgery is performed under local anaesthesia, so no pain is felt during the procedure. In the hours that follow, as the anaesthetic wears off, moderate discomfort or pain in the operated area is normal and easily controlled with common painkillers such as paracetamol or ibuprofen. Most patients report less post-operative discomfort than expected. Swelling and bruising are possible but usually mild and resolve within a few days.
How much does an immediately loaded implant cost?
The cost of immediate-loading treatment varies considerably: number of implants, complexity of the case, need for additional regenerative procedures, type of prosthesis and quality of the materials. For a single implant with a ceramic crown, costs range roughly from 1,500 to 3,000 euros. For full-arch fixed rehabilitations, costs generally fall between 8,000 and 15,000 euros per arch.
What are the success rates of immediate loading?
Success rates for immediate-loading implantology are very high and comparable to delayed loading when the correct patient-selection criteria are respected. The international literature reports success rates between 95% and 98% at 5 years for healthy non-smoking patients. In appropriate cases, immediate loading is a predictable, reliable technique.
Is immediate or delayed loading better?
No technique is universally superior: each has its own specific indications. Immediate loading is preferable when the right anatomical and clinical conditions exist, because it offers shorter treatment times, immediate aesthetic recovery and fewer procedures. Delayed loading remains the more conservative, safer choice with poor bone quality, inadequate primary stability or significant risk factors. The decision belongs to the surgeon after careful case assessment.
Conclusions and Next Steps
Immediate-loading implantology is an advanced, effective solution for replacing lost teeth, when applied in clinically appropriate cases. As we have seen, it offers real advantages in treatment time, immediate aesthetic recovery and lower psychological impact. Yet it demands careful candidate selection and meticulous surgical planning to deliver predictable, lasting results.
The key to success lies in personalising the treatment: every patient has different anatomy, health conditions and expectations that must be carefully weighed. There are no rigid protocols to apply universally, only guidelines to adapt case by case in the spirit of custom regeneration.
If you are considering immediate-loading implantology, or simply want to understand whether it suits your specific case, I invite you to book an evaluation visit at my practice. During the initial consultation we will examine your clinical situation together with appropriate diagnostic exams and discuss the most suitable therapeutic options, explaining benefits, risks and available alternatives.
You can contact the Dentipiu.it dental practice to arrange an appointment and receive a personalised evaluation. The first visit is essential to build a tailored treatment plan that respects your anatomy, your health and your expectations.
Remember: a healthy, functional smile can last a lifetime with the right care and preventive attention. Investing in quality implantology, performed by qualified professionals with certified materials, is an investment in your long-term well-being.
References
- Hamilton A, Gonzaga L, Amorim K, et al. Selection criteria for immediate implant placement and immediate loading for single tooth replacement in the maxillary esthetic zone: A systematic review and meta-analysis. Clin Oral Implants Res. 2023;34(Suppl 26):304-348. doi:10.1111/clr.14109. PMID: 37750515.
- Qin R, Chen Y, Han C, Wu D, Yu F, He D. Immediate Implant Placement With or Without Immediate Provisionalization in the Maxillary Esthetic Zone: A Systematic Review and Meta-analysis. Int J Oral Maxillofac Implants. 2023;38(3):422-434. doi:10.11607/jomi.10112. PMID: 37279220.
- Donker VJJ, Raghoebar GM, Slagter KW, Hentenaar DFM, Vissink A, Meijer HJA. Immediate implant placement with immediate or delayed provisionalization in the maxillary aesthetic zone: A 10-year randomized trial. J Clin Periodontol. 2024;51(6):722-732. doi:10.1111/jcpe.13971. PMID: 38454548.
- Wang Z, Li S, Chen H, Guo L. Efficacy of immediate loading compared to conventional loading in implant-supported removable prostheses: a systematic review and meta-analysis. Acta Odontol Scand. 2024;83:553-563. doi:10.2340/aos.v83.42027. PMID: 39352227.
FAQ
- How long does an immediately loaded implant last?
- An immediately loaded dental implant, once properly integrated and maintained with good oral hygiene, can last a patient's lifetime. The literature reports survival rates above 95% at 10 years for immediately loaded implants in healthy patients. Longevity depends mainly on general health, home and professional hygiene, control of risk factors such as smoking, and regular follow-up visits.
- Can I eat right after immediate-loading surgery?
- Yes, but with important precautions. In the first 24 hours it is best to stick to cold or room-temperature foods that are soft and require no chewing, such as ice cream, yoghurt, smoothies and purees. From 24 hours up to about three weeks, you can chew soft foods carefully while avoiding the operated area. After the first month, when osteointegration is well advanced, a normal diet can be gradually resumed.
- What is the main difference between immediate and delayed loading?
- The key difference lies in the timing of the prosthesis. In immediate loading, the temporary prosthesis is placed within 24-48 hours of implant insertion, giving the patient immediate aesthetic and functional recovery. In delayed loading, complete osteointegration (3-4 months) is awaited before loading the implants. The choice depends on the primary stability achieved at insertion and the patient's anatomy.
- When is immediate loading not possible?
- Immediate loading is not indicated when adequate primary stability cannot be achieved at implant insertion. This typically happens with low-density bone, after recent bone grafts not yet consolidated, in patients with severe uncontrolled bruxism, in heavy smokers unwilling to quit, in decompensated diabetics or in the presence of active infection at the site.
- Is immediate loading painful?
- Immediate-loading surgery is performed under local anaesthesia, so no pain is felt during the procedure. In the hours that follow, as the anaesthetic wears off, moderate discomfort or pain in the operated area is normal and easily controlled with common painkillers such as paracetamol or ibuprofen. Most patients report less post-operative discomfort than expected. Swelling and bruising are possible but usually mild and resolve within a few days.
- How much does an immediately loaded implant cost?
- The cost of immediate-loading treatment varies considerably: number of implants, complexity of the case, need for additional regenerative procedures, type of prosthesis and quality of the materials. For a single implant with a ceramic crown, costs range roughly from 1,500 to 3,000 euros. For full-arch fixed rehabilitations, costs generally fall between 8,000 and 15,000 euros per arch.
- What are the success rates of immediate loading?
- Success rates for immediate-loading implantology are very high and comparable to delayed loading when the correct patient-selection criteria are respected. The international literature reports success rates between 95% and 98% at 5 years for healthy non-smoking patients. In appropriate cases, immediate loading is a predictable, reliable technique.
- Is immediate or delayed loading better?
- No technique is universally superior: each has its own specific indications. Immediate loading is preferable when the right anatomical and clinical conditions exist, because it offers shorter treatment times, immediate aesthetic recovery and fewer procedures. Delayed loading remains the more conservative, safer choice with poor bone quality, inadequate primary stability or significant risk factors. The decision belongs to the surgeon after careful case assessment.
- What are the pros and cons of immediate-loading implantology?
- The pros are concrete: the patient leaves the office with fixed teeth within 24-48 hours, avoids months of removable provisionals, faces one surgery instead of two, and recovers aesthetics and function at once. The cons should not be hidden. Immediate loading works only if the implant achieves sufficient primary stability at insertion: it needs good-quality bone and rigorous case selection. Where those conditions are missing — rarefied bone, recent grafts, uncontrolled bruxism, heavy smoking, decompensated diabetes — forcing immediate loading exposes the patient to early failure that delayed loading would avoid. A real advantage in the right cases, a wrong choice in the wrong ones. The difference is clinical judgement, not the technique itself.
References
Looking for a specialist?
Chirurgia Orale a Frosinone →Espansione di cresta, rialzo del seno mascellare, estrazioni complesse
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stai valutando un impianto dentale?
Ho scritto una guida in 8 capitoli che spiega tutto quello che un paziente dovrebbe sapere prima di sedersi in poltrona. Niente marketing — solo fatti, casi studio e una checklist per fare le domande giuste.
Scarica la guidaStay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment