Periodontitis and Pregnancy: A Link Most People Ignore

In brief — Periodontitis increases preterm birth risk 1.5-fold, low birth weight 2.5-fold, and preeclampsia risk over 3-fold. Oral pathogens colonise the placenta through haematogenous and direct routes, with implications that demand preconceptional periodontal screening and treatment.
Periodontitis increases the risk of preterm birth 1.5-fold. That of low birth weight 2.5-fold. That of preeclampsia over 3-fold. These are not hypotheses. They are data from meta-analyses on over 2.5 million women, published between 2022 and 2025.
Yet how many expectant mothers receive a periodontal assessment before or during pregnancy? How many gynaecologists ask their patient if her gums bleed?
It is true that there are already many pathophysiological variables to monitor during gestation. Nevertheless, oral health should always be considered.
The mechanism has been known for twenty years
Periodontal bacteria reach the placenta. This is not theory. It has been demonstrated by genetic sequencing: the placental microbiome resembles the oral microbiome more than the vaginal or intestinal one.
There is a clear affinity between the two environments, however anatomically distant.
Fusobacterium nucleatum and Porphyromonas gingivalis are the main culprits. The former uses a protein called Fap2 to bind specifically to placental tissues. The latter has been found in 41% of umbilical cords from preterm deliveries, versus much lower percentages in term deliveries.
In 2022, a case report showed what can happen in extreme cases: a woman with mild gingivitis developed fulminant sepsis from periodontal pathogens, with foetal death at 23 weeks. Fusobacterium nucleatum was isolated from the foetal lungs. It had caused necrotising chorioamnionitis.
Other oral bacteria detected in the placenta and amniotic fluid include Capnocytophaga gingivalis, Listeria monocytogenes, Tannerella forsythia, Treponema denticola, Peptostreptococcus micros, Streptococcus sanguis and Aggregatibacter actinomycetemcomitans.
Whether these bacteria can also cause preterm birth or other complications is not yet clear.
Two pathways of damage
The first is direct. Bacteria enter the bloodstream during chewing, brushing, or dental procedures. Or they simply reach the vessels through tissue colonisation mechanisms. Those equipped with specific surface adhesins colonise the placenta. There they multiply and trigger local infection.
The second is indirect. The cytokines produced in the periodontal pocket — IL-1β, IL-6, TNF-α — enter the bloodstream. They reach the feto-placental unit. They stimulate prostaglandin production. PGE2 matures the cervix, ruptures the membranes, initiates contractions.
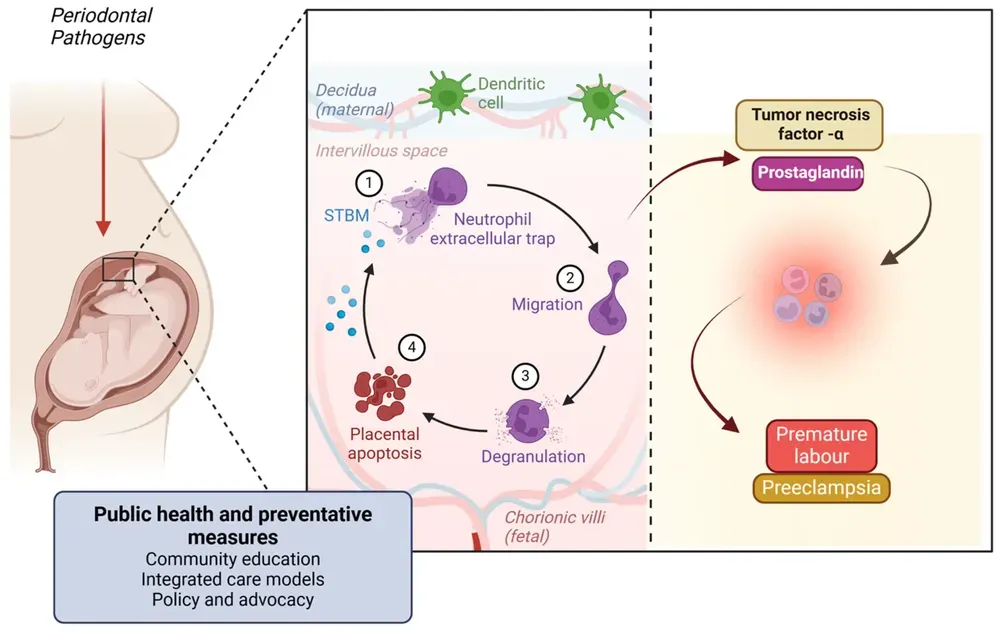
Women with periodontitis and elevated PGE2 levels in amniotic fluid at 15–20 weeks have a 20-fold (!) increased risk of preterm birth compared to normal.
Treating during pregnancy is not enough
Here lies the paradox. The association between periodontitis and adverse outcomes is solid. But treating periodontitis during pregnancy does not consistently reduce these outcomes.
The Cochrane meta-analysis of 15 randomised trials found no significant differences for preterm birth. A reduction exists for low birth weight, but the evidence is of low quality.
A 2024 network meta-analysis found that scaling and root planing alone does not work. It works better if combined with chlorhexidine. But even this combination is no guarantee.
Why? Probably because we arrive too late. By the time a woman discovers she is pregnant and begins prenatal visits, bacteria may have already colonised the placenta. The biological window for intervention is before conception.
The risk factors everyone knows (and the one they ignore)
Obstetric medicine has identified dozens of risk factors for adverse pregnancy outcomes. Some are not modifiable: maternal age, ethnicity, foetal genotype, a previous preterm birth. Others are partially modifiable: gestational diabetes, hypertension, obesity.
The gynaecologist asks whether the patient smokes. Asks about alcohol or drug use. Measures blood pressure. Checks blood glucose. Prescribes folic acid. Assesses cervical length in at-risk pregnancies. Screens for bacterial vaginosis. Treats urinary tract infections.
All correct. All in the guidelines.
But periodontitis? Silence.
Yet periodontitis is different from other risk factors. It is completely modifiable. Treatment is simple, safe, non-invasive. It requires no medication. It has no side effects. Non-surgical treatment is inexpensive. And it affects 40% of women of childbearing age.
Let us compare the numbers. Bacterial vaginosis increases preterm birth risk approximately 2-fold. Periodontitis 1.5 to 2.5-fold. Both are infections. Both are treatable. But for vaginosis there is a recommended screening in at-risk pregnancies. For periodontitis, nothing.
Gestational diabetes increases the risk of macrosomia and neonatal complications. It is actively sought with the glucose tolerance test. Periodontitis increases preeclampsia risk over 3-fold. It is not sought at all.
The difference is not scientific. It is cultural. The mouth is not part of pregnancy. The dentist is not on the prenatal team. Oral health is not real health. But why? Why do we continue to behave as if the mouth were detached from the rest of the body?
What Italian guidelines say
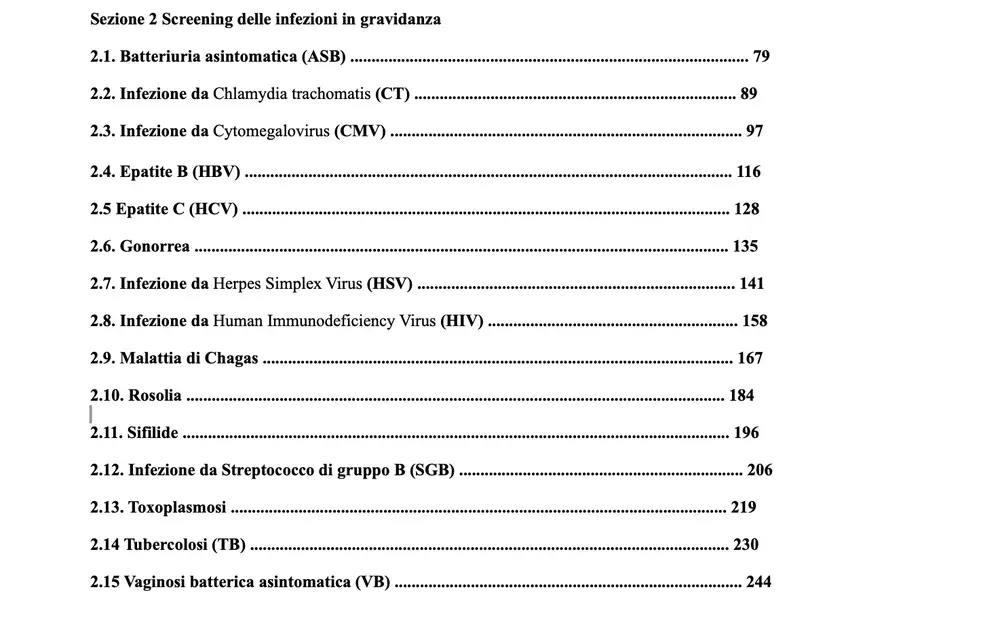
I have read the national SNLG guidelines on physiological pregnancy. Both parts, over 500 pages of recommendations declared to be evidence-based, published in 2023 and 2025.
They contain very important screenings for a long series of infectious diseases: asymptomatic bacteriuria, Chlamydia, cytomegalovirus, hepatitis B, hepatitis C, gonorrhoea, herpes, HIV, rubella, syphilis, group B streptococcus, toxoplasmosis, tuberculosis, bacterial vaginosis.
They also recommend screening for anaemia, haemoglobinopathies, perinatal depression, and, rightly, domestic violence.
The word “periodontitis” does not appear. Ever. In 500 pages.
The word “dental” appears once: as a risk factor for hepatitis B.
Exegetical note: (The usual 1930s cliché. A pity that the data are based on the question "have you ever been to the dentist?". It would be like asking someone with gonorrhoea if they have ever taken a bus. I can already see the headlines: "Gonorrhoea Transmitted by Bus Seats!" In fact, the safety of dental practices has been demonstrated even recently by the very low spread of Covid-19 within them, as opposed to what happened in all other healthcare settings.)No recommendation on oral health. No referral to a dentist for a check-up. No gingival screening. (With rare exceptions of enlightened physicians, as always.)
Let us take as an example one screening recommended in the guidelines: bacterial vaginosis. Vaginosis increases the risk 2-fold. Periodontitis 1.5 to 2.5-fold. For one there is a recommendation. For the other, silence.
Yet periodontitis is at least the sixth most frequent infectious disease in the world (though according to recent studies this figure may be greatly underestimated).
The failure of compartmentalised medicine
Here is the critical point. Periodontitis affects approximately 60% of the world’s population and 40% of women of childbearing age. The link with adverse pregnancy outcomes is documented by hundreds of studies. I have written about this relationship between teeth and general health elsewhere as well.
Yet the majority of practitioners seem to forget that this infectious disease exists.
It would be enough to ask “have you had a dental check-up?”.
And yet, even the guidelines of the American Dental Association and the American College of Obstetricians and Gynecologists agree: periodontal treatment during pregnancy is safe. It can be performed in any trimester. But nobody prescribes it routinely.
The European Federation of Periodontology recommends non-surgical periodontal therapy even during pregnancy.
What should be done
A woman planning a pregnancy should receive a comprehensive periodontal assessment.
If she has periodontitis, she should be treated before conception. Not during. Before.
During pregnancy, periodontal maintenance should be part of the prenatal protocol. Not an optional extra. Not something the patient must request. Part of the protocol.
Gynaecologists should learn to recognise the obvious signs of periodontitis during the history: gingival bleeding, halitosis, tooth mobility. And they should refer the patient to a dentist, or preferably, to a periodontist.
But this would also require the dismantling of certain ideological walls.
It would require that physicians and dentists talk to each other amicably. It would require interdisciplinary training. It would require someone to admit that the mouth is part of the body.
Conclusion
The data are there. The mechanisms are clear. Oral pathogenic bacteria, if they develop excessively, can colonise the placenta. The systemic inflammation triggered by periodontitis reaches the foetus. The risk of preterm birth, low birth weight and preeclampsia increases.
What is missing is action. Awareness is missing in the medical profession. Integration between disciplines is missing. The courage is missing to tell women the truth: your oral health also influences your baby’s health.
Killer 32
I have already addressed this topic, together with the other links between periodontal and general health, in my book Killer 32.
References
Bi WG, Emami E, Luo ZC, Santamaria C, Wei SQ. Effect of Periodontal Treatment in Pregnancy on Perinatal Outcomes: A Systematic Review and Meta-Analysis. J Matern Fetal Neonatal Med. 2021;34(19):3259-3268. [https://doi.org/10.1080/14767058.2019.1678142]
Bonasoni MP, Comitini G, Pati M, et al. Fulminant Sepsis and Perinatal Death at 23 Weeks Due to Fusobacterium nucleatum. Pediatr Dev Pathol. 2023;26(3):456-463. [10.1080/15513815.2022.2131487]
Castaño-Suárez, L., Paternina-Mejía, G.Y., Vásquez‑Olmos, L.D. et al. Linking Periodontitis to Adverse Pregnancy Outcomes: a Comprehensive Review and Meta-analysis. Curr Oral Health Rep 11, 125–137 (2024). [https://doi.org/10.1007/s40496-024-00371-6]
Ghosh A, Jaaback K, Boulton A, et al. Fusobacterium nucleatum: An Overview of Evidence, Demi-Decadal Trends, and Its Role in Adverse Pregnancy Outcomes. Cells. 2024;13(8):717. [https://doi.org/10.3390/cells13080717]
Iheozor-Ejiofor Z, Middleton P, Esposito M, Glenny AM. Treating periodontal disease for preventing adverse birth outcomes in pregnant women. Cochrane Database Syst Rev. 2017;6:CD005297. [https://doi.org/10.1002/14651858.cd005297.pub3]
Le QA, Akhter R, Coulton KM, et al. Periodontitis and Preeclampsia in Pregnancy: A Systematic Review and Meta-Analysis. Matern Child Health J. 2022;26(12):2419-2443. [https://doi.org/10.1007/s10995-022-03556-6]
Merchant AT, Gupta RD, Akonde M, et al. Association of Chlorhexidine Use and Scaling and Root Planing With Birth Outcomes: A Systematic Review and Meta-analysis. JAMA Netw Open. 2022;5(12):e2247632. [https://doi.org/10.1001/jamanetworkopen.2022.47632]
Parhi L, Abed J, Shhadeh A, et al. Placental colonization by Fusobacterium nucleatum is mediated by binding of the Fap2 lectin to placentally displayed Gal-GalNAc. Cell Rep. 2022;38(12):110537. [https://doi.org/10.1016/j.celrep.2022.110537]
Vanterpool, Sizzle F et al. “Porphyromonas gingivalis within Placental Villous Mesenchyme and Umbilical Cord Stroma Is Associated with Adverse Pregnancy Outcome.” PloS one vol. 11,1 e0146157. 5 Jan. 2016, [https://doi:10.1371/journal.pone.0146157]
Tang L, Chen K. Association Between Periodontitis and Adverse Pregnancy Outcomes: Two-Sample Mendelian Randomisation Study. Int Dent J. 2024;74(6):1397-1404. [https://doi.org/10.1016/j.identj.2024.05.001]
Wu J, Wu J, Tang B, et al. Effects of different periodontal interventions on the risk of adverse pregnancy outcomes: a systematic review and network meta-analysis. Front Public Health. 2024;12:1373691. [https://doi.org/10.3389/fpubh.2024.1373691]
Zhang Y, Feng W, Li J, Cui L, Chen ZJ. Periodontal Disease and Adverse Neonatal Outcomes: A Systematic Review and Meta-Analysis. Front Pediatr. 2022;10:799740. [https://doi.org/10.3389/fped.2022.799740]
FAQ
What is the impact of periodontitis on pregnancy and newborns?
How does periodontitis affect pregnancy outcomes?
Why does treating periodontitis during pregnancy not reduce adverse outcomes?
What do Italian pregnancy guidelines say about oral health?
What can be done to improve oral health in women of childbearing age?
References
- https://doi.org/10.1001/jamanetworkopen.2022.47632
- https://doi.org/10.1002/14651858.cd005297.pub3
- https://doi.org/10.1007/s10995-022-03556-6
- https://doi.org/10.1007/s40496-024-00371-6
- https://doi.org/10.1016/j.celrep.2022.110537
- https://doi.org/10.1016/j.identj.2024.05.001
- https://doi.org/10.1080/14767058.2019.1678142
- https://doi.org/10.1080/15513815.2022.2131487
- https://doi.org/10.1111/jcpe.12732?urlappend=%3Futm_source%3Dresearchgate.net%26utm_medium%3Darticle
- https://doi.org/10.3389/fped.2022.799740
- https://doi.org/10.3389/fpubh.2024.1373691
- https://doi.org/10.3390/cells13080717
Looking for a specialist?
Parodontologia a Frosinone →Diagnosi e trattamento della parodontite nello Studio Denti Più
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment