Titanium, Heavy Metals, and the Great Semantic Fraud

Or: how to sell a ceramic implant by scaring the patient with high-school chemistry.
Let’s start with something that needs to be said right away, before anyone takes offence: ceramic implants are excellent. They have some peculiar characteristics, especially on the prosthetic side. But they work. In certain rare cases — such as the extremely uncommon patient with a documented allergic history — they may be the best choice. This article is not against zirconia. It is against the lies told about titanium in order to sell it.
Because the problem is never the product. The problem is the method. And the method of so-called “biological” dentistry is always the same: take a fear, inflate it until it looks like a certainty, and then offer the solution — which, coincidentally, costs more.
Personally, the first implants I ever encountered were, in fact, ceramic. They are nothing new to me. They were beautiful, but had some structural issues. Still, if a patient needs them, I am happy to oblige: no problem at all. The placement technique is the same. But some clarity is needed in this media swamp.
The magic words: “heavy metals”
Open any “biological” dentistry website and sooner or later you will find this sentence: titanium is a heavy metal. Said with the gravity of someone revealing a secret that conventional dentists — “those sell-outs paid by implant companies as part of the great titanium conspiracy” — are hiding from you.
There are many problems with these reckless claims. A fundamental one concerns the very “scientific” definition of the alleged hazard.
IUPAC — the International Union of Pure and Applied Chemistry, the only body in the world with the authority to define what is what in chemistry — published in 2002 a Technical Report whose title is already a verdict: “Heavy Metals” — A Meaningless Term? (Duffus JH, Pure Appl Chem, 2002;74(5):793-807).
The report concludes that the term “heavy metal” has never been coherently defined by any authoritative scientific body. Over more than sixty years of use, it has been given such a wide range of meanings as to become, in effect, meaningless. But above all — and this is where it gets interesting — the report denounces a specific tendency: the unsupported assumption that all so-called “heavy metals” and their compounds are highly toxic. This assumption, writes IUPAC, has no basis in chemical or toxicological data.
In plain English: when someone tells you that titanium is a “toxic heavy metal”, they are using a term that official chemistry considers meaningless, to attribute a property that toxicology does not recognise.
It is a bit like saying your dog is dangerous because it is a “wild animal”. Technically it is an animal, yes. But the word “wild” does not mean what it might seem. And whoever uses it does so precisely to confuse.
What science actually says about titanium
Titanium has been used in medicine and dentistry for over sixty years. Its biocompatibility is not an opinion: it is the result of thousands of studies, millions of implants placed, and decades of clinical follow-up.
Nicholson (2020), in a comprehensive review of titanium alloys for dental implants, concludes that commercially pure titanium (cpTi) and Ti-6Al-4V offer clinical success rates of up to 99% at ten years, with excellent biocompatibility with both bone and gingival tissues. The conclusion is unequivocal: these materials will continue to be used for dental implants in the foreseeable future. Not much room for conspiracy theories.
A 2024 meta-analysis in Clinical Oral Investigations (Kupka et al.) — the first to systematically analyse 20-year data — reports survival rates of 88–92%, with crestal bone loss of less than 1 mm between the first and twentieth year of follow-up. Twenty years of data. Not an Instagram post.
But there is a detail that makes the “toxic heavy metal” narrative even more grotesque. When titanium comes into contact with air or biological fluids, it spontaneously develops an oxide layer — titanium dioxide, TiO₂ — within nanoseconds. This passive layer is what gives titanium its corrosion resistance and biocompatibility. The human body never comes into contact with metallic titanium. Never. What touches the bone, the mucosa, the tissues — is TiO₂. Which is, for all intents and purposes, a ceramic. Anyone fleeing from titanium to take refuge in ceramics is therefore fleeing from one ceramic to embrace another. The irony writes itself.
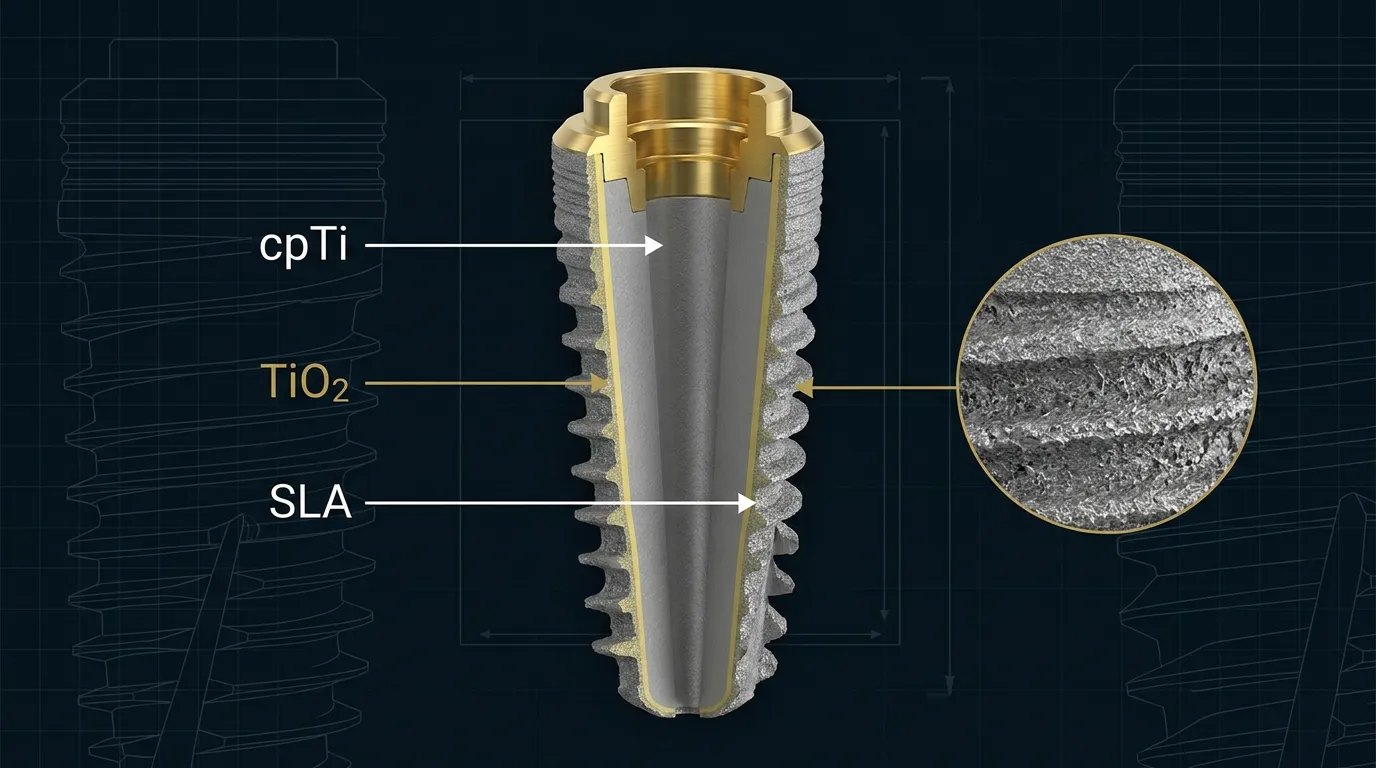
Surface treatments
On top of this, modern implantology has developed surface treatments specifically to optimise the implant–tissue interface. Surfaces such as SLA (Sandblasted, Large-grit, Acid-etched) modify the topography of the oxide layer, increasing roughness and wettability to promote plasma protein adhesion and osteoblastic activity. The result is faster and more predictable osseointegration. We are not talking about a raw piece of metal shoved into the bone — we are talking about surface engineering calibrated to the nanometre. But explaining this requires study. Scaring people with the words “heavy metal” requires only a website.
Not all titanium is created equal
There is a distinction that those who shout “heavy metal” never make — and that any serious professional should know. Not all implant titanium is the same. In Italy and most of Europe, manufacturers use grade 4 titanium: commercially pure titanium (cpTi), with a purity above 99%. No aluminium, no vanadium, no alloys. Just titanium. It is the material chosen by companies that care about the quality of their products, selected precisely for its excellent biocompatibility.
Grade 5 — the Ti-6Al-4V alloy, containing 6% aluminium and 4% vanadium — is used by several manufacturers, including many Israeli ones. Grade 5 offers superior mechanical properties, greater fatigue and fracture resistance, making it suitable for narrow-diameter implants or high-load situations. But it introduces two elements — aluminium and vanadium — that could theoretically raise some discussion about ionic release, although long-term clinical data remain reassuring for both grades.
If “biological” dentists were truly concerned about metallurgical composition — and not simply interested in selling a more expensive alternative — they should at least distinguish between titanium grades. But no. For them it is all “toxic heavy metal”, full stop. Because nuance does not sell. Fear does.
For completeness: there is also the titanium-zirconium alloy (TiZr, marketed by Straumann as Roxolid), which completely eliminates aluminium and vanadium while offering mechanical properties superior to grade 4. An option that makes the “heavy metals in the alloy” argument even more irrelevant.
Titanium allergy: the truth, the whole truth
“Biological” dentistry loves to talk about titanium allergy. And here one must be honest: titanium allergy exists. It is not an invention. But proportions matter. And it may not even be a “true” allergy.
The estimated prevalence is 0.6–1.0% of the population. Poli et al. (2021), in a systematic review in Materials, confirm that titanium should not be considered a completely inert material, but that the incidence of allergic reactions is low. The reactions are mediated by type IV hypersensitivity — a delayed immune response mediated by T lymphocytes.
Watanabe et al. (2023) add an important detail: in many of the cases reported as “titanium allergy”, patients simultaneously tested positive for nickel, mercury, chromium and cobalt. This raises a legitimate question: are we truly dealing with titanium allergy, or with patients who have a multiple allergic predisposition (polyallergic or atopic)? If so, it would not be a true allergy at all, but a generic hyperreactivity to any element or compound.
Furthermore: there is no definitive diagnostic method for titanium allergy. Patch tests and MELISA/LTT show inconsistent results. Diagnosis remains clinical, presumptive, and requires interpretive caution.
So yes, the titanium-allergic patient potentially exists. But they are extremely rare and not easy to identify with certainty.
Confirming all of this, the most up-to-date systematic review on the topic — Restelli et al. (2026), published in the Journal of Prosthodontic Research — screened 1,761 studies and included only 9. Nine studies in the entire world literature. Twenty-one patients, 33 implants. Of these, 20 cases were diagnosed as titanium hypersensitivity, and in 17 the implant had to be removed. The numbers speak for themselves: after decades of titanium implantology on millions of patients, the evidence for hypersensitivity comes down to a handful of case reports.
The authors further note that titanium microparticles found in peri-implant tissues derive mainly from mechanical wear during surgical placement — not from any alleged systemic “toxicity” of the material. These particles may act as immunological co-factors in predisposed individuals, but do not constitute a primary cause of peri-implant inflammation. A subtle but fundamental distinction.
What about ceramics? Let’s talk seriously
Zirconia implants are a valid and evolving option. But the scientific literature — the real kind — tells a somewhat different story from that of “biological” websites.
Padhye et al. (2023), in a systematic review and meta-analysis in Clinical Oral Investigations, compare zirconia and titanium and find no statistically significant differences in survival at 12 months. Good. But the success rates reported in the study vary widely: 57.5–93.3% for zirconia versus 57.1–100% for titanium. And above all: long-term data for zirconia simply do not exist yet.
Afrashtehfar et al. (2020), in a meta-review in the Journal of Prosthetic Dentistry, analyse nine systematic reviews and conclude that zirconia’s clinical outcomes are similar or inferior to those of titanium, with non-homogeneous primary studies, weak methodology, and results described as merely promising in the short term.
Sales et al. (2023), in the Journal of Stomatology, Oral and Maxillofacial Surgery, confirm: no advantage for zirconia over titanium. On the contrary, a favourable difference for titanium in marginal bone loss (p = 0.001). The only area where zirconia shines is aesthetics — the pink aesthetic score — because it does not create the gingival greyness that titanium can produce in thin biotype (but which only appears with incorrect positioning).
Fernandes et al. (2022) find that among titanium, titanium-zirconium (TiZr) and zirconia, the worst survival rate belongs to zirconia (87.5–91.25%), versus 92.6–100% for titanium and 95.8–100% for TiZr.
In summary: zirconia is a promising material, with real aesthetic advantages, but with a still-young body of evidence and results that, for now, do not surpass titanium. If anything, the opposite seems to be the case. Anyone selling it to you as “the safe alternative to the toxic heavy metal” is doing marketing, not science.
The anatomy of the fraud
This is how it works. The pattern is always the same, whether the topic is amalgam, root canals, fluoride or titanium implants.
First: take a scientific term and use it out of context. “Heavy metal” sounds menacing, evoking mercury, lead, arsenic. That titanium has nothing to do with any of those is a detail conveniently omitted.
Second: cite real studies but extrapolate them. Can titanium release particles? Yes, it can. Like any implant material. Zirconia included — the hydrothermal ageing of zirconia is a well-studied and documented phenomenon. But they do not tell you that.
Third: offer the solution. The “metal-free”, “biocompatible” (as if titanium were not), “natural” ceramic implant (as if an industrially manufactured zirconia cylinder were more natural than an industrially manufactured titanium cylinder).
And the circle closes. Fear, omission, sale.
What a serious dental surgeon should say
A serious dental surgeon should tell the truth, which is complex and therefore harder to sell.
Titanium is the implant material with the longest track record in the history of medicine. Sixty years of data, survival rates above 95% at ten years, biocompatibility documented by thousands of peer-reviewed studies in high-impact journals. It is not a heavy metal in the toxicological sense — and that term, in any case, has no accepted scientific definition.
Zirconia is a valid alternative, particularly in the rare case of documented titanium hypersensitivity. But long-term data are insufficient, success rates for now do not exceed those of titanium, and marginal bone loss appears to be greater.
The choice between the two should be based on clinical indications, site anatomy, specific aesthetic needs and, where appropriate, allergy testing — not on fear of “heavy metals”.
Anyone who scares you to sell you something is not practising medicine. They are practising sales.
References
- Duffus JH. “Heavy metals” — a meaningless term? (IUPAC Technical Report). Pure Appl Chem. 2002;74(5):793-807.
- Kupka JR, König J, Al-Nawas B, Sagheb K, Schiegnitz E. How far can we go? A 20-year meta-analysis of dental implant survival rates. Clin Oral Investig. 2024;28(10):541.
- Nicholson JW. Titanium Alloys for Dental Implants: A Review. Prosthesis. 2020;2(2):100-116.
- Poli PP et al. Titanium Allergy Caused by Dental Implants: A Systematic Literature Review and Case Report. Materials. 2021;14(18):5239.
- Watanabe M et al. Are Allergy-Induced Implant Failures Actually Hypersensitivity Reactions to Titanium? A Literature Review. Dent J. 2023;11(11):263.
- Padhye NM et al. Survival and success of zirconia compared with titanium implants: a systematic review and meta-analysis. Clin Oral Investig. 2023;27(11):6279-6290.
- Afrashtehfar KI, Del Fabbro M. Clinical performance of zirconia implants: A meta-review. J Prosthet Dent. 2020;123(3):419-426.
- Sales PHH et al. Do zirconia dental implants present better clinical results than titanium dental implants? A systematic review and meta-analysis. J Stomatol Oral Maxillofac Surg. 2023;124(1S):101324.
- Fernandes PRE et al. Clinical Performance Comparing Titanium and Titanium–Zirconium or Zirconia Dental Implants: A Systematic Review of Randomized Controlled Trials. Dent J. 2022;10(5):83.
- Restelli L, Uriarte X, Moreno X, Mena C, Fernández E, Fan S, Díaz L. Titanium hypersensitivity in dental implants: A systematic review of updated clinical evidence and diagnostic strategies. J Prosthodont Res. 2026. doi:10.2186/jpr.JPR_D_25_00255.
FAQ
- Is titanium a heavy metal?
- No. IUPAC (International Union of Pure and Applied Chemistry) established in 2002 that the term 'heavy metal' lacks a coherent scientific definition and does not imply toxicity. Titanium is not toxic in the toxicological sense of the term.
- Are titanium implants safe in the long term?
- Yes. Titanium has been used in medicine for over sixty years. A 20-year meta-analysis (Kupka et al., 2024) reports survival rates of 88–92%, with crestal bone loss under 1 mm. Biocompatibility is documented by thousands of peer-reviewed studies.
- Is titanium allergy common?
- It is very rare. The estimated prevalence is 0.6–1.0% of the population. The most up-to-date systematic review (Restelli et al., 2026) found only 21 patients worldwide with documented titanium hypersensitivity in dental implants.
- Are ceramic (zirconia) implants better than titanium?
- No, not based on current data. Meta-analyses show similar or inferior results for zirconia compared to titanium, with long-term data still insufficient and marginal bone loss statistically greater in some studies.
- What is the difference between grade 4 and grade 5 titanium?
- Grade 4 is commercially pure titanium (>99%), used by most European manufacturers. Grade 5 (Ti-6Al-4V) contains 6% aluminium and 4% vanadium, offers superior mechanical properties and is often used for narrow-diameter implants.
Looking for a specialist?
Implantologia a Frosinone →Impianti dentali, carico immediato e rigenerazione ossea
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stai valutando un impianto dentale?
Ho scritto una guida in 8 capitoli che spiega tutto quello che un paziente dovrebbe sapere prima di sedersi in poltrona. Niente marketing — solo fatti, casi studio e una checklist per fare le domande giuste.
Scarica la guidaStay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment