Occlusal Trauma Does Not Prevent Periodontal Healing
In brief — Lindhe and Ericsson (1976) demonstrate in a dog model that jiggling-type occlusal trauma does not impair periodontal healing after surgery, provided plaque is removed and hygiene maintained. The periodontal ligament adapts to forces — it widens, it vascularizes — but epithelial and connective tissue attachment heals normally. Plaque infection, not occlusion, is the determining factor.
A question that spanned the twentieth century
For decades, periodontology was divided over a seemingly simple question: does occlusal trauma contribute to periodontal destruction?
On one side, Glickman and the Boston school argued that excessive occlusal forces altered the pathway of gingival inflammation, diverting it towards the periodontal ligament and producing infrabony pockets and angular defects (Glickman & Smulow, 1965). On the other, Waerhaug in Oslo denied any causal role for occlusion, attributing everything to plaque and its apical extension along the root surface (Waerhaug, 1979).
In between, Jan Lindhe and the Gothenburg school were building the answer with the rigour of experimental method.
Study design
The study by Lindhe and Ericsson, published in 1976 in the Journal of Clinical Periodontology, is an experiment on five Beagle dogs conducted with precise sequential logic (Lindhe & Ericsson, 1976).
Day 0: induction of experimental periodontitis. Incision into the periodontal ligament, removal of marginal bone, application of copper bands followed by cotton floss ligatures to promote plaque accumulation. Soft diet. Within six months, the result was an experimental periodontal lesion with marked horizontal bone loss, apical migration of the junctional epithelium, and suprabony pockets.
Day 180: introduction of jiggling-type occlusal trauma. Cap splints with oblique planes on the maxilla and lingual bars with springs on the mandible. Each masticatory cycle pushed the mandibular fourth premolar in a mesio-buccal direction; the spring returned it to position. Alternating, continuous, measurable forces. Within one hundred days, the trauma produced angular bony defects and infrabony pockets — the co-factor described by Glickman took shape in the experimental model.
Day 280: the decisive moment. On one side (control), trauma was eliminated, pockets were treated with a modified Widman flap, teeth were scaled, and oral hygiene was initiated twice daily. On the other side (test), everything was identical — except that trauma persisted. The jiggling continued.
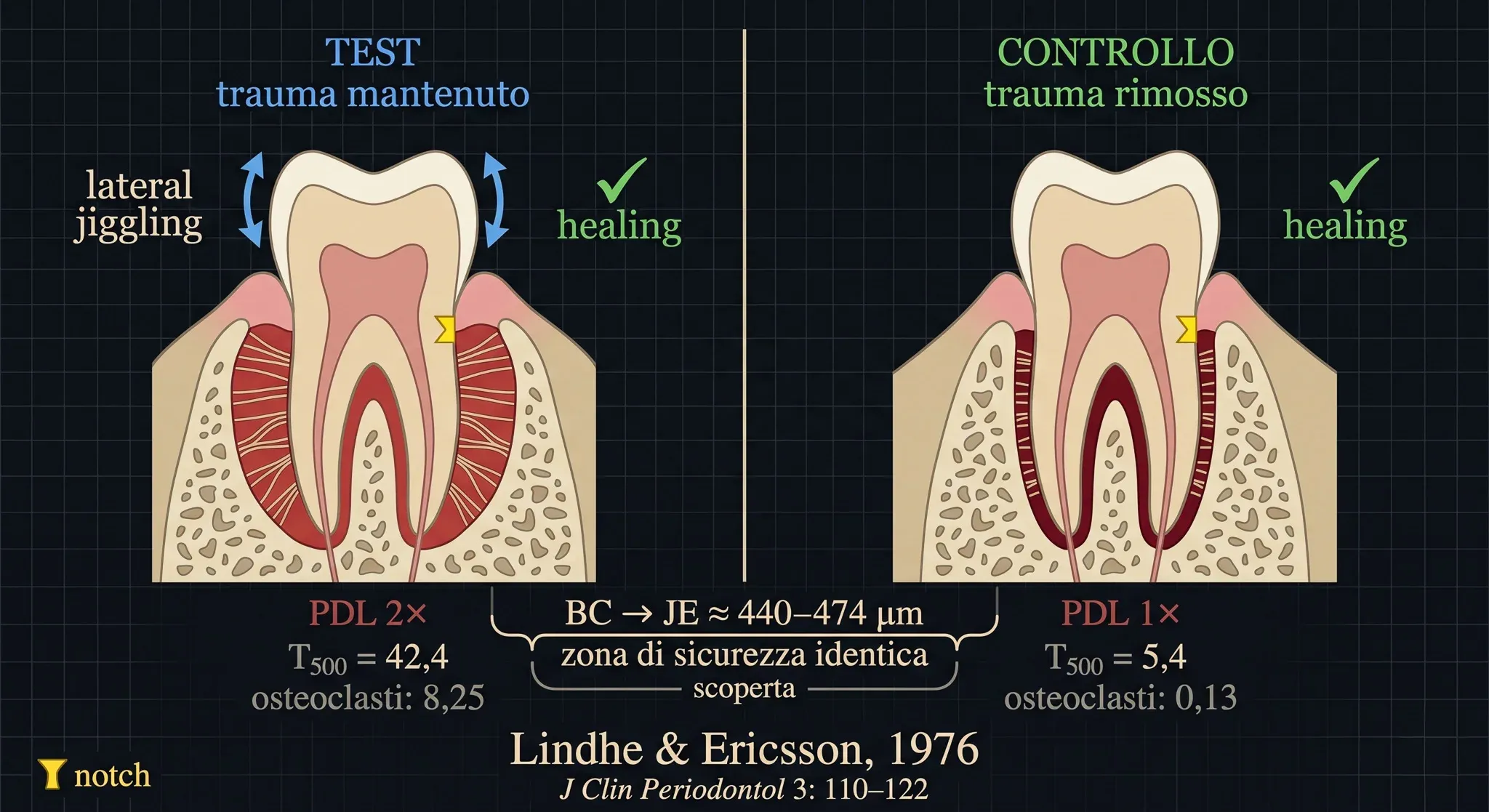
A crucial detail: during surgery, a reference notch was cut into the root at the level of the pocket floor. This would serve as the zero point for histological measurements.
Day 370: radiographs, histological sections, microscopic analysis.
What the data show
The results are unequivocal.
In control teeth — trauma removed — mobility returned to baseline values. The periodontal ligament narrowed, the alveolar crest appeared distinct and radiopaque on radiographs, the junctional epithelium was smooth, the connective tissue free of inflammatory infiltrate. Complete healing.
In test teeth — trauma maintained — mobility continued to increase (T₅₀₀ = 42.4 versus 5.4 in controls). The periodontal ligament area was twice as wide. The vascular cross-section area was twice as large. The number of osteoclasts on the bone surface was sixty times higher (8.25 vs 0.13).
And yet — and this is the finding that matters — healing occurred. Entirely independent of occlusal trauma.
The junctional epithelium — with its hemidesmosomes perfectly adhered — was smooth, without rete pegs. The supra-alveolar connective tissue was free of inflammatory infiltrate. Collagen fibres inserted into newly formed cementum apical to the junctional epithelium — that biological barrier separating the external environment from the deep periodontium. The distance between the bone crest and the junctional epithelium — what Waerhaug called the “safety zone” — was identical in test and control teeth: approximately 440–474 µm.
The tooth was mobile. The ligament was widened. But the tissues were perfectly healthy in the absence of bacteria.
Biological significance
Lindhe and Ericsson demonstrate a fundamental distinction that many still struggle to grasp: functional adaptation is not pathology.
The periodontal ligament subjected to jiggling forces responds with adaptive remodelling. The space widens to absorb the forces. Vascularization increases. Osteoclasts work to remodel bone. This is the traumatic phase described by Svanberg and Lindhe in 1973, followed by the post-traumatic phase in which tissues reach a new equilibrium (Svanberg & Lindhe, 1973).
But this process — ligament widening, increased mobility, bone remodelling — does not prevent regeneration of the supra-alveolar tissues. The epithelium heals. The connective tissue reorganizes. Attachment is re-established.
The key is plaque removal. Once infection is eliminated and adequate hygiene established, healing proceeds regardless of occlusal loading. Trauma is not the engine of destruction: it is an amplifier that functions only in the presence of the signal — the bacterial plaque and its microbial population.
Clinical confirmation
The experimental study by Lindhe and Ericsson did not remain isolated. Nyman, Rosling, and Lindhe had already shown in humans that professional plaque control allowed periodontal healing even in hypermobile teeth subjected to jiggling forces (Nyman et al., 1975; Rosling et al., 1976).
Glickman himself, in earlier work with Smulow, had observed that occlusal trauma did not appear to influence gingival healing after mucogingival surgery (Glickman et al., 1966). The evidence was already there, waiting to be read — but it took Lindhe’s experimental design to make it unequivocal.
Why this study matters
The 1976 study is one of the pillars supporting a clinical principle now firmly established: the absolute priority in periodontal treatment is infection control.
A mobile tooth due to occlusal trauma, in the absence of active inflammation, does not require occlusal adjustment to heal after periodontal surgery. Mobility is a sign of adaptation, not disease progression. Occlusal intervention has specific indications — interferences compromising function, patient discomfort, progressive mobility — but it is not a prerequisite for soft tissue healing.
This does not mean occlusion is irrelevant. It means that in the causal hierarchy of periodontal disease, bacterial plaque comes first. Always.
Fifty years on: has anyone refuted Lindhe?
No. And it is worth understanding why.
The most authoritative recent work is the narrative review by Fan and Caton, produced for the 2017 AAP/EFP World Workshop on periodontal disease classification and published simultaneously in the Journal of Periodontology and the Journal of Clinical Periodontology (Fan & Caton, 2018). The conclusions, after reviewing all available literature, are identical to Lindhe’s: occlusal trauma does not initiate periodontitis or connective tissue attachment loss. When plaque-induced periodontitis and trauma coexist, the evidence that trauma accelerates attachment loss is defined as weak.
The only recent study that might appear contradictory is a retrospective case-control by Ríos et al. involving 372 patients, which finds an association between occlusal trauma and periodontitis (Ríos et al., 2021). But a retrospective case-control does not establish causation, and the risk of reverse causality is obvious to anyone who treats periodontitis daily: it is periodontal disease that causes tooth migration and occlusal discrepancies, not the other way around.
To refute Lindhe and Ericsson would require another controlled experiment demonstrating the opposite — that periodontal healing does not occur in the absence of plaque but in the presence of trauma. No one has produced such evidence in fifty years. Not because no one has tried, but because the data keep saying the same thing.
An experiment that speaks clearly
The work of Lindhe and Ericsson belongs to that rare category of studies that settle a debate. Not with opinions, not with case series, but with a controlled experimental design where every variable is isolated and measurable.
Fifty years later, the message remains identical: remove plaque, control infection, maintain hygiene. The rest — forces, mobility, ligament width — is biology adapting. A functional adaptation, not a pathology.
FAQ
Does occlusal trauma cause periodontitis?
Can a mobile tooth heal after periodontal surgery despite ongoing occlusal trauma?
What is jiggling-type occlusal trauma?
What is the primary factor in periodontal destruction?
Does the periodontal ligament return to normal after trauma removal?
Is the Lindhe and Ericsson study still valid today?
References
- https://doi.org/10.1002/JPER.16-0581
- https://doi.org/10.1002/JPER.20-0598
- https://doi.org/10.1111/j.1600-051X.1979.tb02185.x
- https://doi.org/10.1902/jop.1966.37.4.319
- PubMed 1064595
- PubMed 1069012
- PubMed 1094035
- PubMed 14261862
- PubMed 4518200
- https://pubmed.ncbi.nlm.nih.gov/14261862/
- https://pubmed.ncbi.nlm.nih.gov/1064595/
- https://pubmed.ncbi.nlm.nih.gov/4518200/
- https://pubmed.ncbi.nlm.nih.gov/1094035/
- https://pubmed.ncbi.nlm.nih.gov/1069012/
Go deeper
Espansione crestale (split crest) →Allargare la cresta senza trapianto — tecnica ERE e bonebending
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment