The Art of the Laterally Repositioned Flap
In brief — The laterally repositioned flap is a minimally invasive procedure that exploits secondary intention healing to naturally regenerate keratinized tissue around implants without autologous grafts. Cells migrate from wound margins and fill the space with tissue of identical anatomic and functional quality.
Regenerate without grafts: is it possible?
Do you always need a graft to widen the keratinized mucosa around dental implants? Probably not — not if you use a laterally repositioned flap.
The procedure rests on cellular healing toward the centre of the incised tissue. A “natural” augmentation of the site.
Cells migrate from the margins and “fill the void” with new tissue of the same quality.
The phenomenon is well known in nature. It is called healing by secondary intention.

From mistake to strategy: secondary intention
Healing by secondary intention has, historically, a negative connotation. In poorly sutured wounds or surgical incisions where edges do not meet, secondary intention occurs by accident — a mistake, sometimes leading to healing defects such as keloids. In most cases, then, the goal is precise flap adaptation to obtain healing by “first intention” instead.
In periodontal and implant surgery, however, secondary intention healing can be a powerful ally, precisely because of its inherent regenerative capacity.
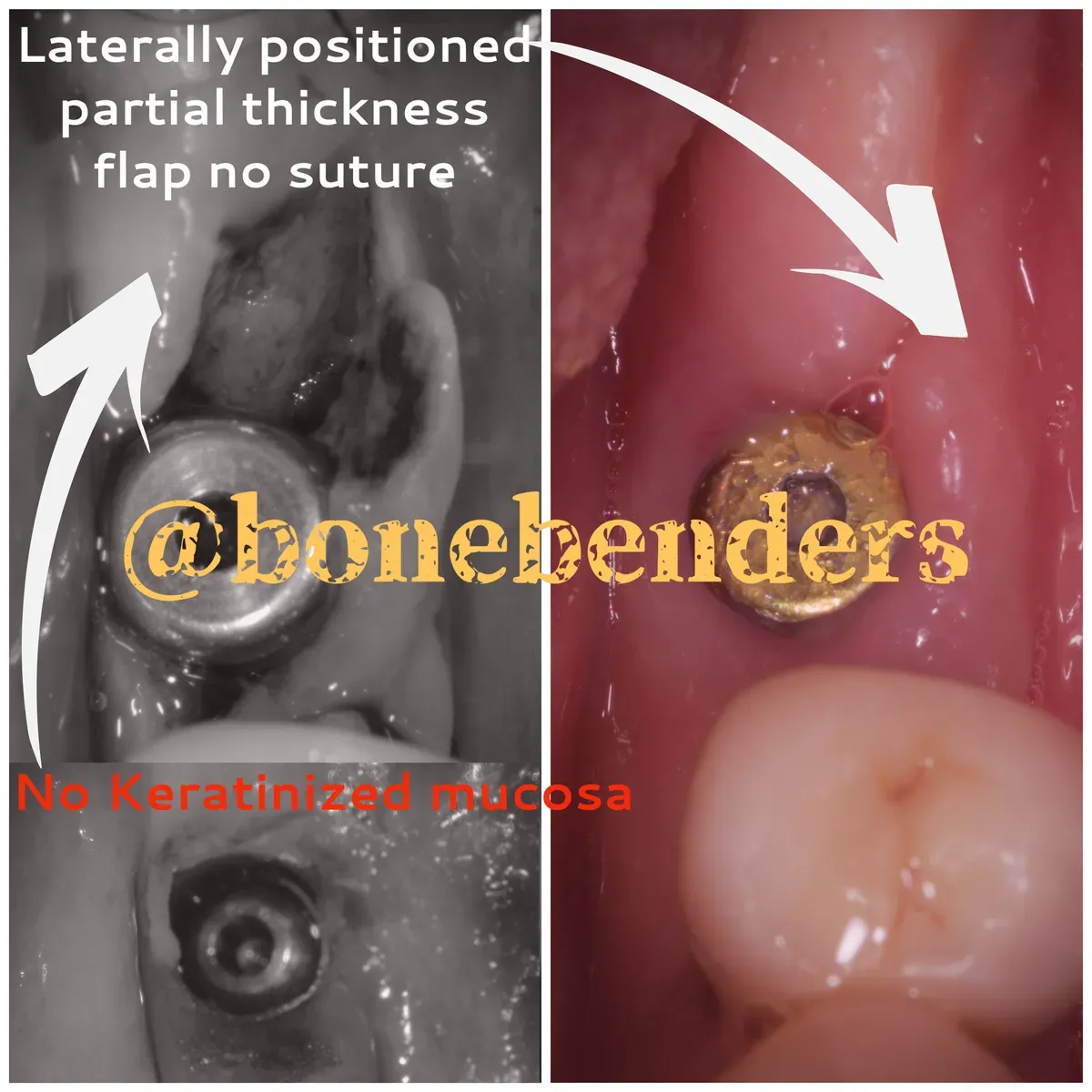
In the clinical case shown below, the laterally repositioned flap, left deliberately open and unsutured, achieves full regeneration of the peri-implant keratinized mucosa — now universally recognized as essential for preventing peri-implant mucositis and peri-implantitis.
The threshold now accepted is ≥ 2 mm of keratinized mucosa. A 2025 umbrella review of more than 7,000 patients documents that, below this threshold, plaque, inflammation and recession all rise. A 2024 prospective study goes further: in the presence of mucositis, a band narrower than 2 mm reduces the odds of clinical resolution after non-surgical therapy by 80%. Those two millimetres aren’t cosmetic. They are ground.
The clinical outcome
The crowns on these implants end up surrounded by the right kind of tissue — keratinized. The patient can brush without discomfort and is not forced to constantly clean food residue from under the crowns.
Wide keratinized tissue at the base of the prosthetic tooth is necessary to optimize the aesthetic and functional outcome of the restoration. The logic is the same one that drives the whole bonebending philosophy: get bone and keratinized mucosa together, without biomaterials.
The question then flips: do you really need a graft every time? A 2023 systematic review followed augmented sites beyond 36 months: outcomes stay stable in the medium-long term, peri-implantitis incidence remains low (0–7%). It works — but that is no reason to do it across the board. A band of keratinized tissue can also be born on its own, if you give it room and time.
The next image (from the same case as the previous photos) makes these concepts clear.
References
- Ionescu A, et al. Open Healing: A Minimally Invasive Protocol with Flapless Ridge Preservation in Implant Patients. Biology (Basel). 2022;11(1):142. doi:10.3390/biology11010142
- Ríos-Osorio N, Ladino LG, Guerrero-Torres M. Structure, biology, and function of peri-implant soft tissues in health and disease: a comprehensive review of the literature. J Periodontal Implant Sci. 2025;55(5):323-348. doi:10.5051/jpis.2402080104
- Blasi G, Chierico F, Amerio E, et al. Influence of keratinized mucosa width on the resolution of peri-implant mucositis: A prospective cohort study. Clin Implant Dent Relat Res. 2024;26(3):581-591. doi:10.1111/cid.13317
- Fathi A, Salehi S, Kazemi F, Nayerain Jazi S. The Significance of Keratinized Mucosa on Implant Health: An Umbrella Review. J Oral Implantol. 2025;51(4):314-320. doi:10.1563/aaid-joi-D-25-00049
- Stefanini M, Barootchi S, Sangiorgi M, et al. Do soft tissue augmentation techniques provide stable and favorable peri-implant conditions in the medium and long term? A systematic review. Clin Oral Implants Res. 2023;34 Suppl 26:28-42. doi:10.1111/clr.14150
Related reading: surgical treatment of peri-implantitis — TST technique.
FAQ
Is tissue regenerated by the lateral flap stable over time?
Why is this method not better known among dentists?
What is the main advantage compared to autologous grafts?
How much keratinized mucosa can be regenerated with this technique?
What happens if the wound becomes infected?
References
Go deeper
Espansione crestale (split crest) →Allargare la cresta senza trapianto — tecnica ERE e bonebending
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment