In the waiting room the question is always the same. It comes before the chair, sometimes before the diagnosis itself. Doctor, but how much radiation is that?
It’s a good question. It deserves an answer that isn’t just a number tossed out there.
The trouble is that the number, on its own, says nothing. Effective dose is measured in millisieverts, mSv. A dental intraoral X-ray is 0.005 mSv. Five thousandths. To anyone who doesn’t live and breathe medical physics, that figure means nothing: it neither reassures nor frightens. It’s mute.
To make it speak, you have to translate it. And the most honest way is to translate it into time.
The background of the world
We live immersed in radiation. It comes from space, from rocks, from the radon rising out of the ground, from the potassium inside our own bones. It’s the natural background: on average about 3 mSv a year, somewhat less in the worldwide average. We don’t feel it. We can’t switch it off. It’s the fixed price we pay for being in the world.
So the dose of an exam can be read like this: how many days, months or years of that background it adds up to.
A dental intraoral X-ray, 0.005 mSv, is worth about one day. A single day of life on Earth. A panoramic, around 0.025 mSv, three days. A Cone Beam scan depends heavily on the field of view and the machine: for small and medium volumes you stay between 0.08 and 0.2 mSv — a few weeks to a month of background — but with large fields, and on certain units, it climbs considerably. Small numbers, when you look at them up close.
The flight as a yardstick
There’s one comparison that works better than a thousand explanations. Anyone who boards a plane and crosses the ocean, just once, collects at high altitude the cosmic rays that the atmosphere spares us on the ground. A one-way intercontinental leg is worth about 0.05 mSv; a round trip between Europe and New York, around 0.1. Ten times the dose of a dental X-ray, for the sheer pleasure of leaving. And yet nobody, before a trip, wonders how much radiation they’ll pick up up there.
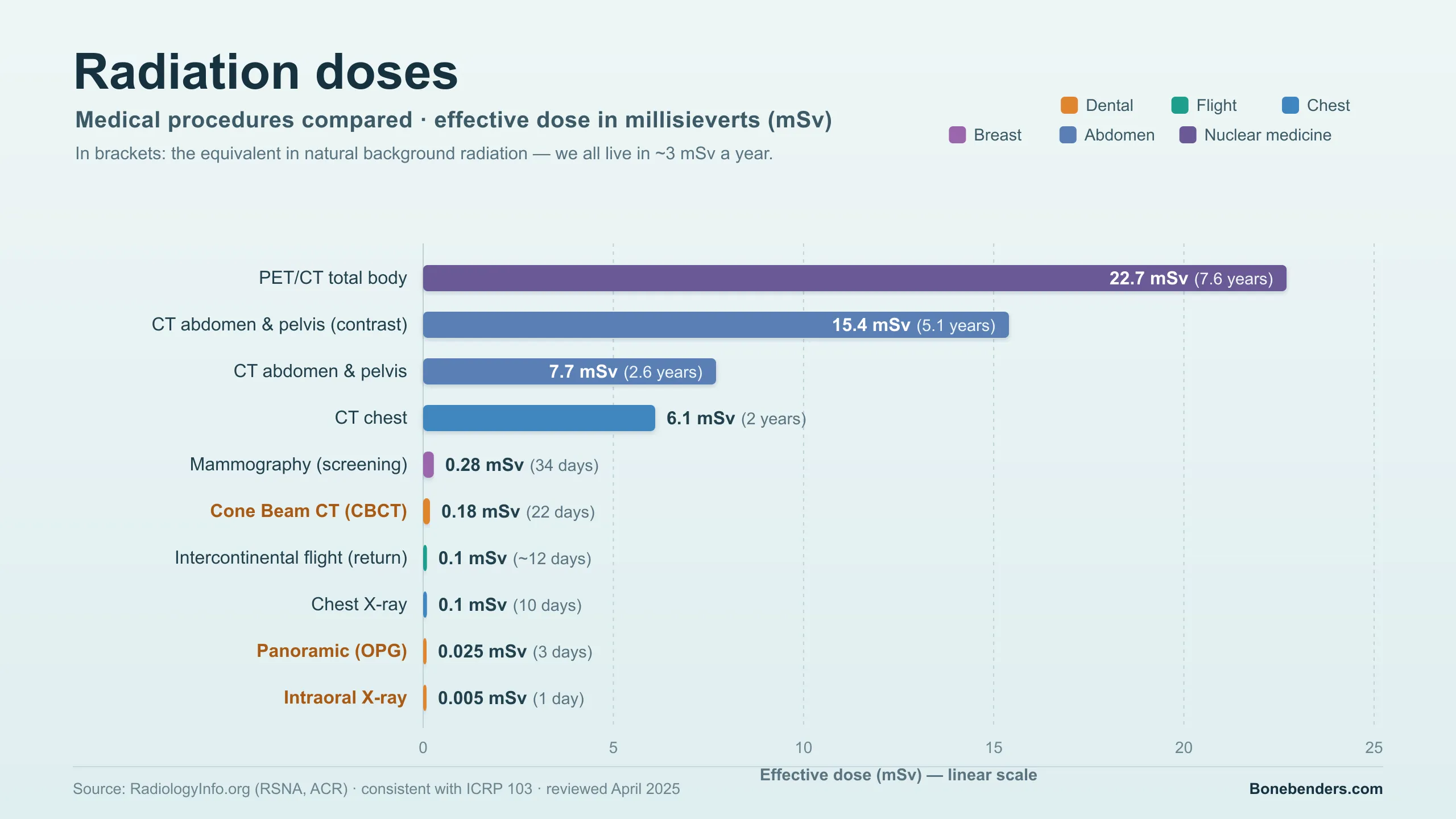
Lined up against the rest of medicine, dental doses shrink to a single line. A chest CT is on the order of 6 mSv, an abdomen-and-pelvis one almost 8, a whole-body PET/CT over 20. Two years of natural background, three, almost eight. It’s another order of magnitude. The intraoral, beside them, all but disappears.
A higher dose doesn’t mean danger
Here we need honesty, because it’s easy to slip. A higher dose is not, in itself, dangerous; a lower one is not automatically harmless. The point isn’t the dose in the absolute: it’s the ratio between the diagnostic benefit and the small risk that every exposure carries with it. A justified X-ray, taken when it’s needed, is worth far more than the millisieverts it costs. A pointless X-ray, however light, is just dose given away.
This is the heart of radiation protection: justify every exam, then optimise it. The International Commission calls it the principle of the reasonably lowest possible dose — the old ALARA, which in radiology has become ALADA: the lowest that still lets us see what we need to see.
For whoever presses the button, this translates into concrete gestures. Rectangular collimation on intraoral X-rays cuts the dose compared with the round cone. On the lead apron, though, radiation protection has changed its mind. In 2023 the American Academy of Oral and Maxillofacial Radiology recommends dropping it as routine practice — gonadal apron and thyroid collar alike. They don’t stop the internal scatter that the body itself generates — almost all the dose that ends up outside the field; if anything they cover what needs to be seen, force retakes, pick up saliva. The real protection lies elsewhere: justify the exam, collimate tightly, choose the technique well. The Cone Beam is prescribed only after the clinical examination, never as screening, and always with the smallest field of view that answers the question. And with children prudence counts double: more sensitive tissues, a longer life ahead, doses to be weighed with care.
Fear and rays
Restoring the proportions isn’t about minimising. It’s about deciding well. The patient who refuses the X-ray they actually need, out of fear, risks more than the one who has it. And the clinician who prescribes one too many, out of habit, betrays the same principle.
In between lies the right measure. One day of background for an intraoral. Three for a panoramic. Less than an intercontinental flight for both.
Fear, sometimes, weighs more than the rays.
The comparison figures between exams are drawn from the RadiologyInfo.org table (RSNA and ACR), consistent with the ICRP 103 recommendations. The chart accompanying this article shows them on a linear scale, with the dental region highlighted and the intercontinental flight as a reference point.
References
- RadiologyInfo.org (RSNA, ACR). Patient Safety — Radiation Dose in X-Ray and CT Examinations. Revised April 2025.
- ICRP. The 2007 Recommendations of the International Commission on Radiological Protection. ICRP Publication 103. Ann ICRP 2007;37(2–4).
- Ludlow JB, Davies-Ludlow LE, White SC. Patient risk related to common dental radiographic examinations: the impact of 2007 ICRP recommendations regarding dose calculation. J Am Dent Assoc 2008;139(9):1237–1243. doi:10.14219/jada.archive.2008.0339. PMID: 18762634.
- Ludlow JB, Timothy R, Walker C, Hunter R, Benavides E, Samuelson DB, et al. Effective dose of dental CBCT—a meta analysis of published data and additional data for nine CBCT units. Dentomaxillofac Radiol 2015;44(1):20140197. doi:10.1259/dmfr.20140197. PMID: 25224586.
- European Commission. Radiation Protection No. 172. Cone Beam CT for Dental and Maxillofacial Radiology: Evidence-Based Guidelines (SEDENTEXCT project). Luxembourg: European Commission; 2012.
- National Council on Radiation Protection and Measurements. Radiation Protection in Dentistry and Oral & Maxillofacial Imaging. NCRP Report No. 177. Bethesda: NCRP; 2019.
- White SC, Scarfe WC, Schulze RKW, et al. The Image Gently in Dentistry campaign: promotion of responsible use of maxillofacial radiology in dentistry for children. Oral Surg Oral Med Oral Pathol Oral Radiol 2014;118(3):257–261. doi:10.1016/j.oooo.2014.06.001. PMID: 25066244.
- Johnson KB, Ludlow JB. Intraoral radiographs: a comparison of dose and risk reduction with collimation and thyroid shielding. J Am Dent Assoc 2020;151(10):726–734. doi:10.1016/j.adaj.2020.06.019. PMID: 32979952.
- Bundesamt für Strahlenschutz (BfS). Cosmic radiation during flights. (Frankfurt–New York round trip ≈ 0.1 mSv.)
- UNSCEAR. Sources and Effects of Ionizing Radiation. UNSCEAR 2008 Report. New York: United Nations; 2010. (Natural background, worldwide average ≈ 2.4 mSv/year.)
- Benavides E, Bhula A, Gohel A, Lurie AG, Mallya SM, Ramesh A, et al. Patient shielding during dentomaxillofacial radiography: recommendations from the American Academy of Oral and Maxillofacial Radiology. J Am Dent Assoc 2023;154(9):826–835. doi:10.1016/j.adaj.2023.06.015. PMID: 37530694.
References
- https://doi.org/10.14219/jada.archive.2008.0339
- https://doi.org/10.1259/dmfr.20140197
- https://doi.org/10.1016/j.oooo.2014.06.001
- https://doi.org/10.1016/j.adaj.2020.06.019
- https://doi.org/10.1016/j.adaj.2023.06.015
- https://pubmed.ncbi.nlm.nih.gov/18762634/
- https://pubmed.ncbi.nlm.nih.gov/25224586/
- https://pubmed.ncbi.nlm.nih.gov/25066244/
- https://pubmed.ncbi.nlm.nih.gov/32979952/
- https://pubmed.ncbi.nlm.nih.gov/37530694/
Looking for a specialist?
Parodontologia a Frosinone →Prevenzione e cura delle malattie gengivali e parodontali
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment