The Groove Nobody Checks: Mesial Concavity and Periodontitis in First Premolars
65% of your upper first premolars have a groove that dental floss will never clean.
There is an anatomical detail that most patients — and more than a few clinicians — overlook. A groove on the root. Small, invisible to the naked eye, almost never visible on a periapical radiograph. But capable of changing the periodontal prognosis of a tooth.
It is called the mesial concavity of the maxillary first premolar. And it is one of those cases where anatomy dictates clinical outcome far more than home hygiene ever could.
An unforgiving anatomy
The mesial surface of the upper first premolar root is not flat. In the vast majority of cases it presents a longitudinal depression — a concavity — starting from the cemento-enamel junction and extending apically. This concavity is not an anomaly. It is the norm.
Chen et al. (2024), in a cross-sectional study in Scientific Reports analysing 343 maxillary first premolars in 226 patients with periodontitis, found a prevalence of 65.6%. But the figure varies enormously across studies: Zhao et al. (2014), in the Journal of Periodontal Research, report 100% prevalence of mesial concavity in maxillary premolars. Beycioglu et al. (2024), in BMC Oral Health, confirm 100% in a sample of 200 teeth. The differences depend on classification criteria, but the message is clear: nearly all upper first premolars have one.
And here lies the problem. A groove present in at least two out of three teeth — and possibly all of them — is not an anatomical curiosity. It is a risk factor.
Why the mesial concavity is a trap
Think about what happens in the patient’s mouth. Food particles lodge in the depression. Bacterial plaque layers in the bottom of the groove, where the toothbrush cannot reach and dental floss slides over without ever touching the concave surface. Calculus forms in a zone that even the hygienist cannot easily see without careful probing.
Chen et al. confirm it with numbers: the plaque index is significantly higher on the mesial side of premolars with concavity. The concave buccal side shows higher rates of bleeding on probing (BOP), signalling a more severe inflammatory state. Clinical attachment loss (CAL) is greater in teeth with pronounced concavity.
It is not the patient’s lack of hygiene. It is the anatomy creating an ecological niche — a micro-habitat where periodontal pathogens thrive undisturbed. The patient can brush three times a day, floss, use a water flosser, rinse with mouthwash. If the concavity is deep and the gingival sulcus is already compromised, it will not be enough.
Depth matters — and CBCT reveals it
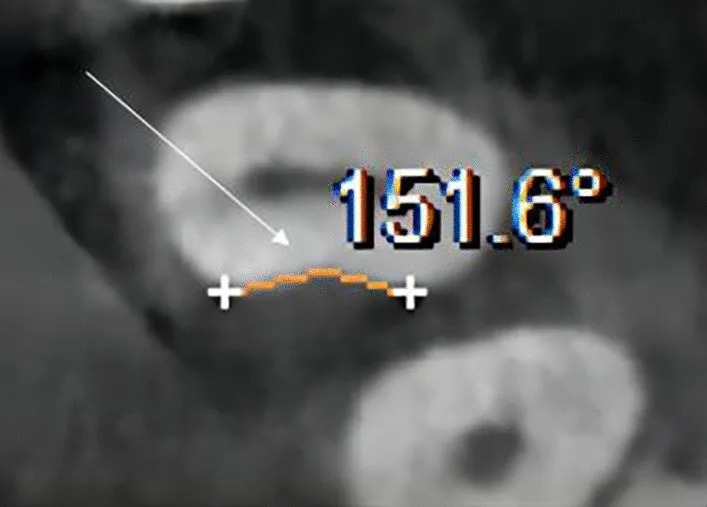
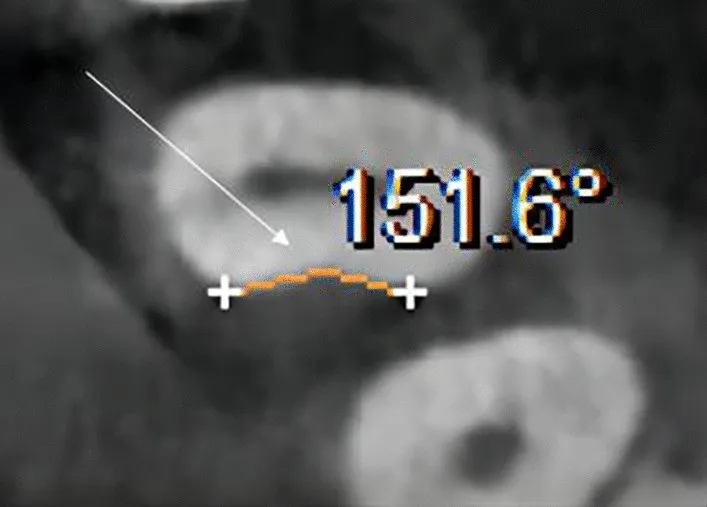
Not all concavities are equal. Chen et al. did something no previous study had attempted: measuring the angle of the concavity at the axial CBCT section. Not just the depth, not just the presence or absence — the angle. A measurement that quantifies how “closed” the groove is and therefore how difficult instrumental access will be.
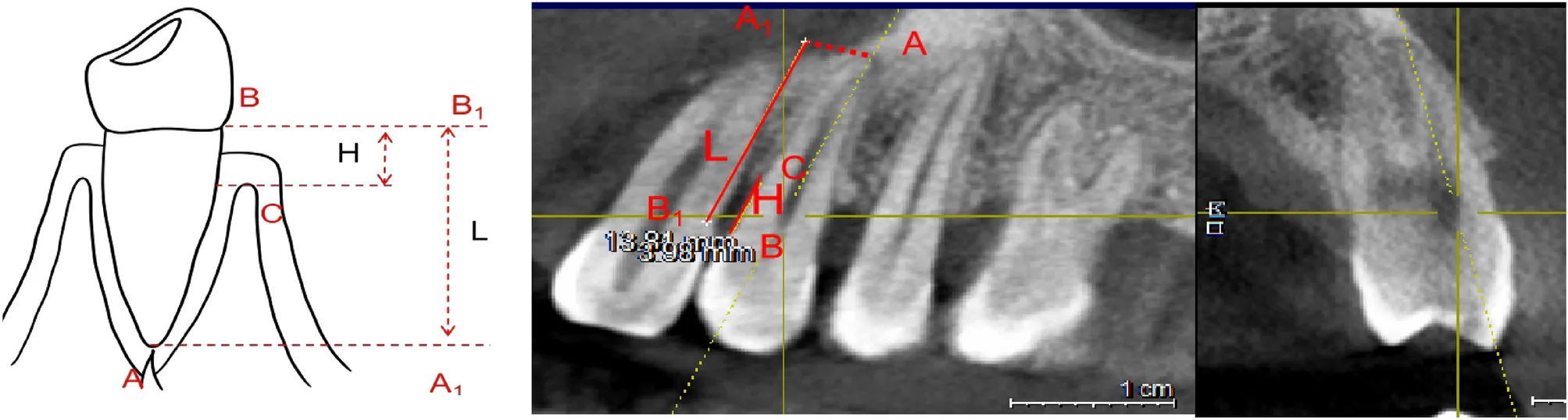
Beycioglu et al. (2024) take the discussion deeper. In 200 maxillary premolars, they find that the starting point of the concavity is in the cervical third of the root in 58.5% of cases — exactly where periodontal bone loss begins. Mean depth is 0.96 mm, but the relevant finding is the correlation: concavity depth is significantly associated with the amount of alveolar bone loss (F = 5.834, p = 0.001). The highest mean depth — 1.29 mm — is found in the group with 50% bone loss.
There is also a finding on furcation: when the root bifurcation is in the cervical third, 100% of patients present bone loss exceeding 50%. When it is in the apical third, only 9.5%. The furcation position amplifies or attenuates the effect of the concavity. Anatomy upon anatomy.
The type of bone defect changes
Zhao et al. (2014) add an observation with direct implications for periodontal therapy. In teeth without mesial concavity, the interproximal bone defect is predominantly ramp-shaped — uniform horizontal resorption. In teeth with concavity, the defect is predominantly crater-shaped — vertical, localised, deeper bone loss.
The difference is not academic. Crater defects respond differently to therapy than ramp defects. They require different surgical approaches. They carry a different prognosis. And if the clinician does not know that the crater is there because root anatomy carved it, they risk attributing disease progression to the patient’s hygiene alone — or worse, to “non-compliance”. When the real culprit is a groove in the root that nobody looked at.
What this means for the clinician
Chen et al. conclude with a recommendation that should become standard practice: the mesial concavity of the upper first premolar must be recognised in diagnosis and treatment planning. It is not an academic detail. It is clinical and must influence the treatment plan.
CBCT, where available, is the instrument of choice — periapical radiography shows the concavity only in two-dimensional projection, without revealing depth or angle. Mesial probing must be interpreted with caution: a deep value on the upper first premolar may not be disease alone. It may be an unfavourable anatomy. The distinction changes the therapy.
And then there is the home hygiene ceiling. Telling the patient “brush better” when the problem is an inaccessible root groove is not therapy. It is buck-passing.
If CBCT shows a deep concavity with a crater-shaped bone defect, non-surgical debridement may not suffice. Regenerative surgery must be planned knowing that root morphology will condition the outcome. Those who do not know the shape of the root they are treating are not making a diagnosis.
But there is good news. The shape can be modified to promote healing and prevent recurrence.
References
- Chen F, Liu Q, Liu X, Fang Q, Zhou B, Li R, Shen Z, Zheng KX, Ding C, Zhong L. Periodontitis was associated with mesial concavity of the maxillary first premolar: a cross-sectional study. Sci Rep. 2024;14(1):2955. doi:10.1038/s41598-024-53371-y. PMID: 38316868.
- Beycioglu Z, Acar B, Ocak M, Bayrakdar IS, Guncu GN, Akman AC. Evaluation of the relationship between periodontal bone destruction and mesial root concavity of the maxillary first premolar. BMC Oral Health. 2024;24(1):735. doi:10.1186/s12903-024-04494-1. PMID: 38926720.
- Zhao H, Wang H, Pan Y, Pan C, Jin X. The relationship between root concavities in first premolars and chronic periodontitis. J Periodontal Res. 2014;49(2):213-9. doi:10.1111/jre.12097. PMID: 23668795.
FAQ
What is the mesial concavity of the maxillary first premolar?
Why does the mesial concavity worsen periodontitis?
How is the mesial concavity diagnosed?
Does the mesial concavity affect bone resorption?
Looking for a specialist?
Parodontologia a Frosinone →Diagnosi e trattamento della parodontite nello Studio Denti Più
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment