Tribocorrosion: a false interface problem, not a titanium defect
Tribocorrosion is real. But with the right connection — conical, Morse taper — or with no connection at all — one-piece, transmucosal implants — it becomes a false problem. The answer isn’t to swap the material for one that seals worse.
Every so often, on social media or at a conference, someone brings up tribocorrosion as the definitive argument against titanium. The clinical experience behind it is often real — thirty years of implants in the mouth — and the observations deserve attention. They also deserve to be separated from the story built on top of them.
Because tribocorrosion is a real phenomenon: documented, studied. And that’s exactly why it can be addressed with data, not with convictions.
What tribocorrosion is — and what it isn’t
Start with the definition. Tribocorrosion is the combination of mechanical wear and electrochemical corrosion that happens when two contacting surfaces slide against each other in a watery environment. In the implant setting, we’re talking about the interface between implant and abutment: under chewing load, the two components micro-slide, generating metal debris and ion release.
Apaza-Bedoya et al. (2017), in a scoping review in the Journal of Periodontal Research, confirm that the presence of microgaps, biofilm and oral fluids at the implant-prosthetic interface causes both mechanical and biological complications. Micro-movements increase wear on the inner surfaces of the connection. The debris released — ions, micro- and nanoparticles — can stimulate peri-implant inflammation.
All true. But watch the subject of the sentence: the problem is the interface, not the material. Tribocorrosion is not an intrinsic defect of titanium. It’s a defect of connection design and of mechanical instability between the components. Any pair of materials — titanium-titanium, titanium-zirconia, titanium-gold alloy — undergoes tribocorrosion if the interface allows micro-movement. Sun et al. (2024), in Dental Materials, showed exactly this by simulating realistic clinical conditions with 5 μm of oscillation amplitude: tribocorrosive damage appears in both Ti-Ti and Zr-Ti pairs, through different mechanisms, but none is exempt.
Presenting tribocorrosion as proof that titanium is dangerous confuses the symptom with the cause. It’s like blaming glass for being fragile because it shatters when you throw it at a wall. The problem is the throw, not the glass.
The conical connection already solved the problem
And here’s where it gets instructive. Modern implantology didn’t just stand by and watch. The solution to tribocorrosion has existed for decades: it’s called the conical connection.
Morse taper connections rely on a simple, powerful mechanical principle: two conical surfaces, forced one into the other, generate a cold weld — a friction fit so tight that the interface becomes functionally monolithic. The residual gap drops below a micron. Mishra and Chowdhary (2017), in a systematic review in the Journal of Clinical and Diagnostic Research that analyzed 30 studies, conclude without ambiguity: the Morse taper connection shows the least microleakage of all the connections tested, under both static and dynamic conditions. And they add a detail worth pausing on: zirconia abutments show greater microleakage than titanium ones.
Ceruso et al. (2017) confirm it: the ideal connection should behave like a one-piece implant, avoiding the formation of a microgap. Internal conical connections manage this. External hexagon connections don’t — they were already failing in static tests.
A gap below a micron sits beneath the threshold that lets most periodontal pathogens through. No micro-movement, no infiltration, no meaningful tribocorrosion. And one-piece transmucosal implants remove the problem upstream: no connection, no interface.
But explaining the engineering of connections takes study. Saying “titanium is the problem” takes only a post.
Why the hybrid implant isn’t the answer
Now for the elephant in the room. Some propose the hybrid implant — a grade 4 titanium body with a transmucosal zirconia collar — as an elegant solution to tribocorrosion. The idea sounds good. Materials physics contradicts it.
Zirconia is a ceramic. Ceramics don’t deform plastically. That’s the point — and it’s a point that allows no rhetorical shortcuts. A zirconia collar cannot achieve the cold weld titanium reaches in a conical connection. Metal adapts, conforms, closes the gap below a micron. Ceramic doesn’t. It wedges in, but it doesn’t seal.
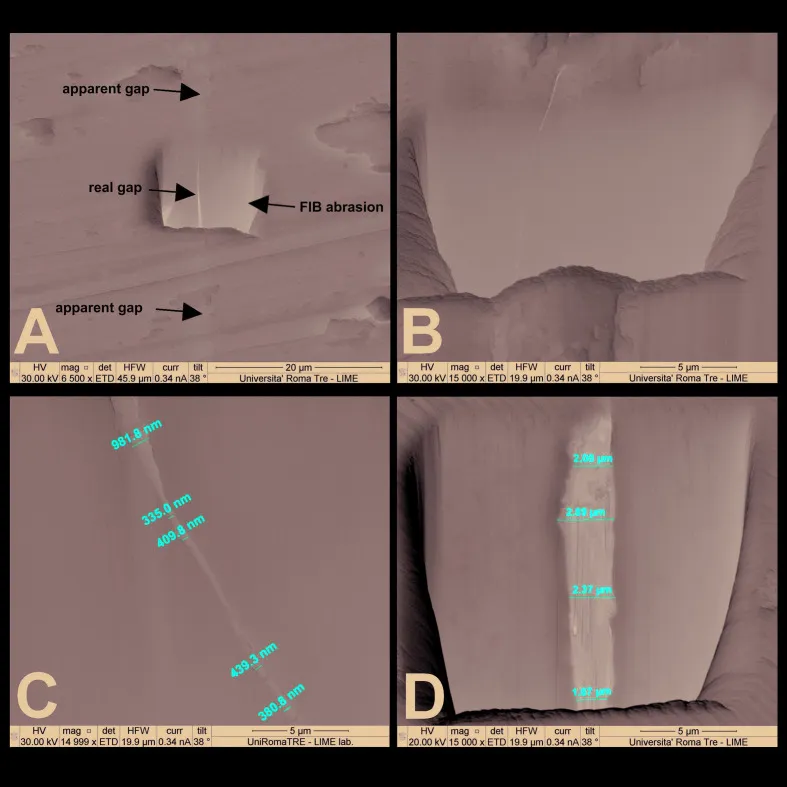
The data confirm it. Abduo and Yin (2018), in a systematic review and meta-analysis in the International Journal of Oral & Maxillofacial Implants, find that zirconia abutments tend to show larger interface gaps and rotational misfits than metal abutments. Sui et al. (2014), in the Journal of Dentistry, measure it directly: the Morse taper microgap between implant and zirconia abutment is 17.55 ± 1.68 μm. Seventeen microns. Not sub-micron. Not a cold weld.
A wider microgap means bacterial infiltration. Bacterial infiltration means peri-implant inflammation. Anyone claiming the hybrid implant guarantees “no mucositis and therefore no peri-implantitis” is promising something the numbers don’t support. An interface that seals worse than titanium-titanium can’t guarantee less bacterial infiltration. It can only guarantee more.
Every material ages — zirconia included
There’s a subtle irony in this whole debate. Those who attack titanium over particle release forget — or prefer not to mention — that zirconia has its own Achilles’ heel: hydrothermal aging.
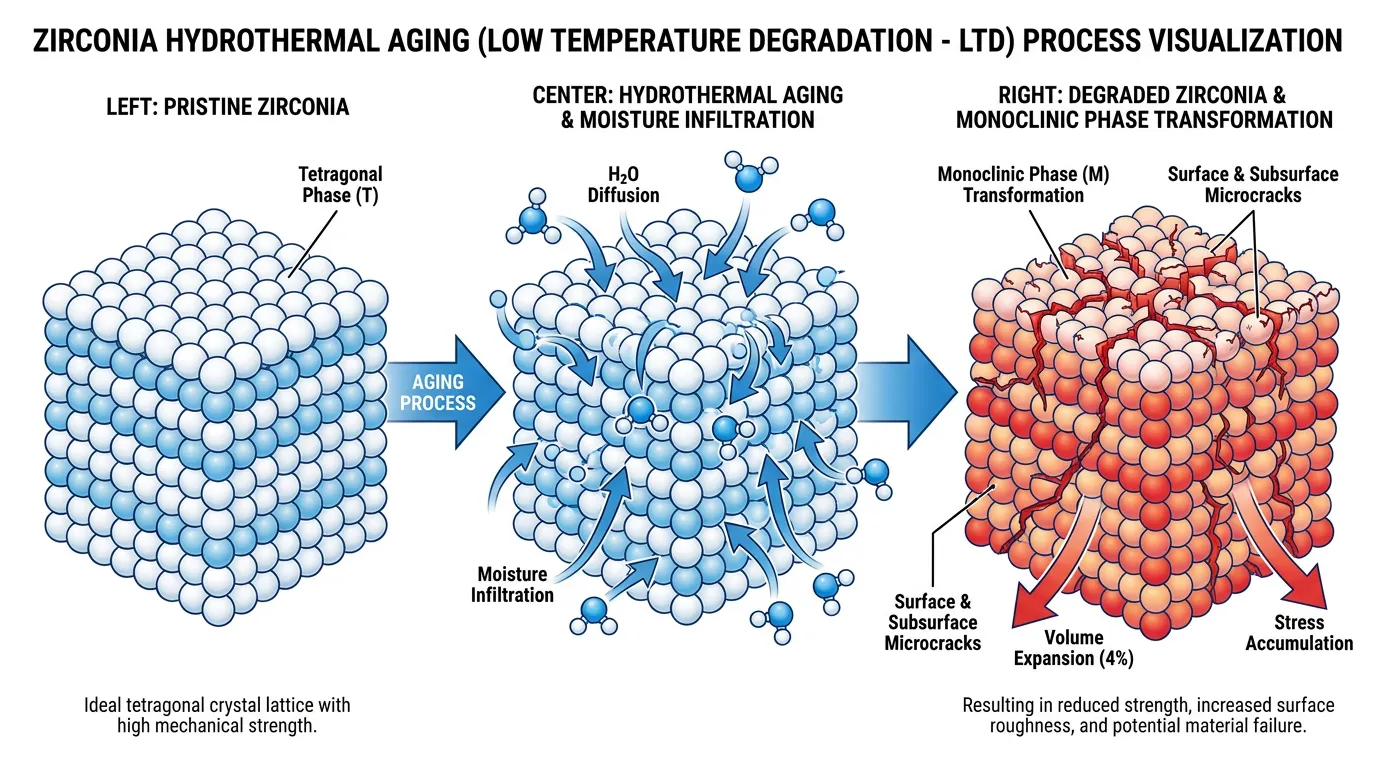
Low Temperature Degradation (LTD) is a well-documented phenomenon in which ambient moisture drives a phase transformation in zirconia: from the tetragonal phase to the monoclinic one. The result is a localized volume increase that generates surface microcracks and degrades mechanical properties over time. Bergamo et al. (2021), in the Journal of the Mechanical Behavior of Biomedical Materials, show it quantitatively: hydrothermal aging raises the monoclinic content by 20–37%, alters the three-dimensional fit of zirconia abutments, and lowers their probability of survival under high loads.
Camposilvan et al. (2015), in Acta Biomaterialia, devote an entire study to finding ways to prevent LTD — proof that the problem is recognized and far from trivial.
But on the sites selling the “hybrid solution,” none of this comes up. Zirconia ages? A negligible detail. Titanium releases particles? A planetary scandal. Two weights, one scale.
Implant fractures: tribocorrosion isn’t the only culprit
Some pin implant fractures on tribocorrosion, as if it were a single, sufficient cause. It isn’t. Fractures are multifactorial: implant diameter, connection design, occlusal loads, bruxism, the crown-to-implant ratio, positioning. Reducing all of it to a single mechanism is an oversimplification the literature doesn’t support.
And zirconia, incidentally, has lower fracture toughness than titanium. Sailer et al. (2018), in the largest systematic review of implant-supported fixed dental prostheses published in Clinical Oral Implants Research, find a five-year survival rate of 93.0% for zirconia prostheses versus 98.7% for metal-ceramics (p < 0.001). 4.1% of zirconia prostheses were lost to framework fracture — against 0.2% of metal-ceramics. Anyone proposing zirconia as the answer to implant fractures is proposing a material that fractures more.
Microparticles: another piece of the puzzle
The most up-to-date systematic review on titanium microparticles — Restelli et al. (2026), published in the Journal of Prosthodontic Research — clarifies a point worth repeating until it enters the conversation: the microparticles found in peri-implant tissues come mainly from mechanical wear during surgical insertion. Not from in situ corrosion. Not from some presumed systemic toxicity of the material.
These particles may act as immunological co-factors in predisposed individuals, but they are not a primary cause of peri-implant inflammation. It’s a subtle distinction, but a fundamental one. And the numbers confirm it: of 1,761 studies screened, only 9 included documented cases of titanium hypersensitivity. Twenty-one patients in the entire world literature.
Alrabeah et al. (2018), in the Journal of Dental Research, add an interesting figure: platform switching significantly reduces the release of tribocorrosive products (p < 0.001). Which suggests, once again, that the problem is manageable through connection design — not through swapping the material.
The solution is engineering, not commercial
To recap. Tribocorrosion is a real interface problem. Conical connections with a cold weld solve it by dropping the microgap below the critical threshold. Monolithic transmucosal implants eliminate it. Platform switching reduces debris release.
The titanium-zirconia hybrid implant, by contrast, introduces an interface that seals worse — because ceramic doesn’t deform plastically — and a material prone to hydrothermal aging. It doesn’t solve the problem: it creates new ones.
Titanium’s twenty-year survival rates stay between 88% and 92% (Kupka et al., 2024). Zirconia, including the hybrid variant, has no comparable long-term data.
This isn’t about defending a material out of loyalty. It’s about not presenting as a “solution” something the data don’t support — and that materials physics contradicts.
The answer to tribocorrosion isn’t a change of material. It’s a change of engineering. Conical connection, adequate torque, platform switching, and when possible: monolithic.
Anyone selling a solution that science doesn’t confirm is doing marketing. Anyone proposing an alternative based on an already-solved problem is confusing chronology with causality.
References
- Apaza-Bedoya K, Tarce M, Benfatti CAM, Henriques B, Mathew MT, Teughels W, et al. Synergistic interactions between corrosion and wear at titanium-based dental implant connections: a scoping review. J Periodontal Res. 2017;52(6):946-954. PMID: 28612506.
- Sun Y, Shukla A, Ramachandran RA, Kanniyappan H, Yang B, Harlow R, et al. Fretting-corrosion at the implant-abutment interface simulating clinically relevant conditions. Dent Mater. 2024;40(11):1823-1831. PMID: 39174418.
- Mishra SK, Chowdhary R, Kumari S. Microleakage at the different implant abutment interface: a systematic review. J Clin Diagn Res. 2017;11(6):ZE10-ZE15. PMID: 28764310.
- Ceruso FM, Barnaba P, Mazzoleni S, Ottria L, Gargari M, Zuccon A, et al. Implant-abutment connections on single crowns: a systematic review. Oral Implantol (Rome). 2017;10(4):349-353. PMID: 29682251.
- Abduo J, Yin L. Fits of implant zirconia custom abutments and frameworks: a systematic review and meta-analyses. Int J Oral Maxillofac Implants. 2018;34(1):99-114. PMID: 30282084.
- Sui X, Wei H, Wang D, Han Y, Deng J, Wang Y, et al. Experimental research on the relationship between fit accuracy and fracture resistance of zirconia abutments. J Dent. 2014;42(10):1353-1359. PMID: 24561040.
- Bergamo ETP, Campos TMB, Lopes ACO, Cardoso KB, Gouvea MVR, de Araújo-Júnior ENS, et al. Hydrothermal aging affects the three-dimensional fit and fatigue lifetime of zirconia abutments. J Mech Behav Biomed Mater. 2021;124:104832. PMID: 34536801.
- Camposilvan E, Marro FG, Mestra A, Anglada M. Enhanced reliability of yttria-stabilized zirconia for dental applications. Acta Biomater. 2015;17:36-46. PMID: 25641645.
- Sailer I, Strasding M, Valente NA, Zwahlen M, Liu S, Pjetursson BE. A systematic review of the survival and complication rates of zirconia-ceramic and metal-ceramic multiple-unit fixed dental prostheses. Clin Oral Implants Res. 2018;29 Suppl 16:184-198. PMID: 30328185.
- Alrabeah GO, Knowles JC, Petridis H. Reduction of tribocorrosion products when using the platform-switching concept. J Dent Res. 2018;97(9):995-1002. PMID: 29578825.
- Kupka JR, König J, Al-Nawas B, Sagheb K, Schiegnitz E. How far can we go? A 20-year meta-analysis of dental implant survival rates. Clin Oral Investig. 2024;28(10):541. PMID: 39305362.
- Restelli L, Uriarte X, Moreno X, Mena C, Fernández E, Fan S, et al. Titanium hypersensitivity in dental implants: a systematic review of updated clinical evidence and diagnostic strategies. J Prosthodont Res. 2026. doi:10.2186/jpr.JPR_D_25_00255. PMID: 41581901.
FAQ
What is implant tribocorrosion?
How is tribocorrosion solved?
Is the titanium-zirconia hybrid implant safer?
Are implant fractures caused by tribocorrosion?
Are titanium microparticles toxic?
References
- https://pubmed.ncbi.nlm.nih.gov/28612506/
- https://pubmed.ncbi.nlm.nih.gov/39174418/
- https://pubmed.ncbi.nlm.nih.gov/28764310/
- https://pubmed.ncbi.nlm.nih.gov/29682251/
- https://pubmed.ncbi.nlm.nih.gov/30282084/
- https://pubmed.ncbi.nlm.nih.gov/24561040/
- https://pubmed.ncbi.nlm.nih.gov/34536801/
- https://pubmed.ncbi.nlm.nih.gov/25641645/
- https://pubmed.ncbi.nlm.nih.gov/30328185/
- https://pubmed.ncbi.nlm.nih.gov/29578825/
- https://pubmed.ncbi.nlm.nih.gov/39305362/
- https://pubmed.ncbi.nlm.nih.gov/41581901/
Looking for a specialist?
Implantologia a Frosinone →Impianti dentali, carico immediato e rigenerazione ossea
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stai valutando un impianto dentale?
Ho scritto una guida in 8 capitoli che spiega tutto quello che un paziente dovrebbe sapere prima di sedersi in poltrona. Niente marketing — solo fatti, casi studio e una checklist per fare le domande giuste.
Scarica la guidaStay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment