
In brief — Chronic bad breath has three main sources: the stomach, the tongue, and the gums. When it comes from the gums, the cause is the periodontal pocket, where periopathogens break down proteins into volatile sulfur compounds that smell of rotten eggs and cabbage. A 2024 meta-analysis put a number on it: people with periodontitis are about four times more likely to have halitosis. The first treatment is not a mouthwash — it is treating the periodontitis itself.
Sintesi (IT) — L’alito cattivo cronico ha tre origini principali: stomaco, lingua e gengive. Quando viene dalle gengive, la causa è la tasca parodontale, dove i periopatogeni producono composti solforati volatili che sanno di uova marce e cavolo. Una meta-analisi del 2024 lo ha quantificato: chi ha la parodontite ha una probabilità circa quattro volte maggiore di soffrire di alitosi. La prima terapia non è un collutorio, ma la cura della parodontite stessa.
Read the title above one more time, and you may become aware of one of the three main causes of bad breath. Among the possible culprits we have to list disorders of the stomach, of the tongue, and also gum disease — periodontitis. For the purposes of this article, we will focus on the periodontal cause.
Picture the pathological environment of the gingival pocket, the signature of periodontal disease, where pathogenic micro-organisms proliferate undisturbed, building up soft and calcified deposits (calculus), and where the bacteria that attack the host’s tissues take up residence.
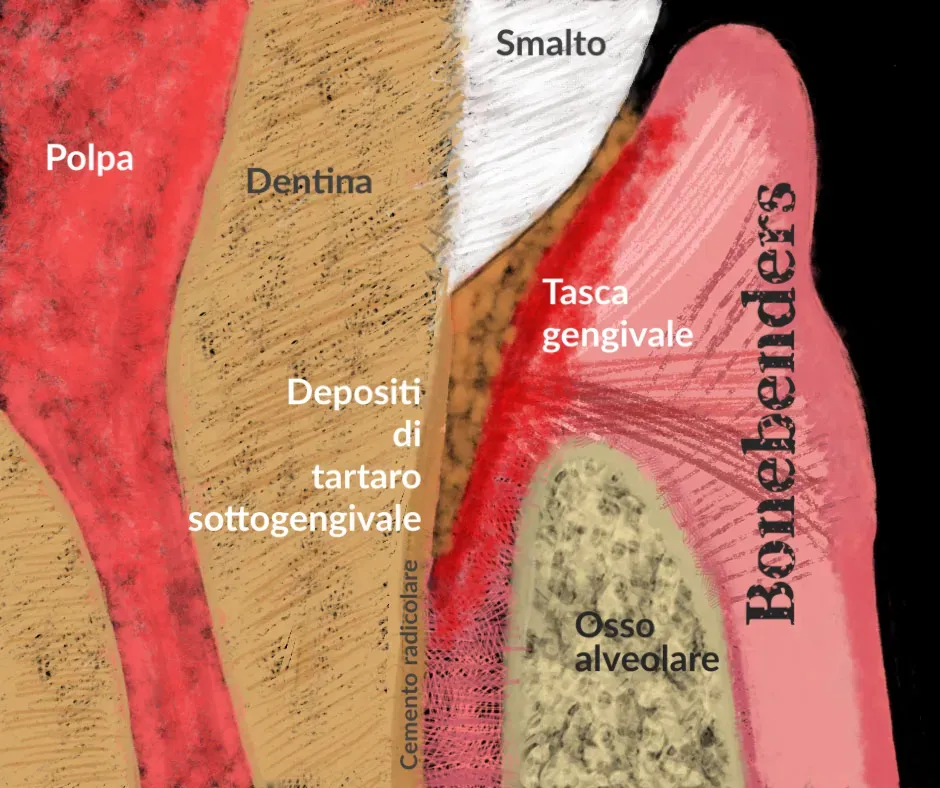
The drawing above illustrates that clinical situation, which can be symptomatic but, more often, is silent.
As these micro-organisms multiply, they create a condition known as dysbiosis. In this state the “bad guys” become dominant over the less harmful bacteria, and they produce an unpleasant smell.
Porphyromonas gingivalis, Prevotella intermedia and Fusobacterium nucleatum are among the most aggressive periopathogens, and they produce a nauseating substance (a smell of faeces, or broccoli) called methanethiol, or methyl mercaptan.
Treponema denticola and Veillonella alcalescens produce hydrogen sulfide, which stinks of rotten eggs.
Most periopathogens form hydrogen sulfide from L-cysteine. Fusobacterium, Prevotella, Porphyromonas and Eubacteria form methanethiol from L-methionine. After incubation in serum, the most powerful hydrogen sulfide producers are Treponema denticola and the black-pigmented species Prevotella intermedia, Prevotella loescheii, Porphyromonas endodontalis and Porphyromonas gingivalis. In serum, Porphyromonas endodontalis and P. gingivalis also produce significant amounts of methanethiol.
No surprise, then, that periodontal disease and halitosis are so tightly linked.
And this is not a clinical impression: it is a number. A systematic review with meta-analysis by Nini and colleagues (Clinical Oral Investigations, 2024), pooling nine studies and more than two thousand people, quantified the link. Someone with periodontitis is roughly four times more likely to have bad breath — whether you measure it with the examiner’s nose, the old organoleptic test, or with the device that counts volatile sulfur compounds. Four times. Not a detail to hide behind a mint.
In patients with deep probing depths and/or significant bleeding-on-probing scores, the ratio of methanethiol to hydrogen sulfide is higher than in those with milder periodontal disease. Total sulfur in deep, inflamed sites is significantly higher than in shallow, non-inflamed sites.
If you have active, untreated periodontal disease, your breath will probably smell of rotten eggs and “cabbage”. So keeping good oral hygiene and treating periodontal disease is essential to make sure your breath smells fresh and clean.
So how do you get rid of that smell? Not with a mouthwash. Or rather: not only with a mouthwash. The origin is inside the pocket, and as long as the pocket stays inflamed the smell comes back, on schedule, every time. The first treatment for periodontal halitosis is the treatment of periodontitis itself: remove the subgingival biofilm, reduce probing depth, treat the disease at its root. Everything else — mouthwashes, tongue scrapers, probiotics — comes afterwards, and works only as an adjunct.
On those adjuncts the literature is honest, and at times it contradicts itself. Light-based therapies — diode lasers and antimicrobial photodynamic therapy — lower volatile sulfur compounds in the short term: Wiench and colleagues confirm it in their 2025 review (Pharmaceutics), while noting the limit straight away — the effect fades within one or two weeks unless you repeat it. On probiotics the verdict swings. A 2022 systematic review (Tay and colleagues, Clinical Oral Investigations) found no convincing benefit; a more recent 2025 one (Passadakis and colleagues) does document a significant VSC reduction in controlled trials. Translated into clinical terms: they may help, but they do not replace the hand that cleans the pocket. A mint covers; it does not cure.
Now, perhaps, you may feel inspired to take steps to deal with any periodontal causes of your bad breath — seeking the support of a professional or, at the very least, adopting a consistent oral hygiene routine. Let these positive feelings of motivation and empowerment flow through you, and know that you have the power to take control of your oral health, with the help of your dental hygienist and your dentist.
Featured image by Mudassar Iqbal from Pixabay.
References
- Nini W, Chen L, Zhang J, Wang L, Yang J. The association between halitosis and periodontitis: a systematic review and meta-analysis. Clin Oral Investig. 2024;28(6):341. doi:10.1007/s00784-024-05732-0 · PMID 38801476
- Wiench R, Fiegler-Rudol J, Zięba N, Misiołek M. Laser interventions for intraoral halitosis: a systematic review of randomized controlled trials. Pharmaceutics. 2025;17(8):1046. doi:10.3390/pharmaceutics17081046 · PMID 40871067
- Passadakis G, Neophytou C, Davidopoulou S, Papadimitriou K. Effectiveness of probiotics in managing oral halitosis: a systematic review of randomized controlled trials. J Int Soc Prev Community Dent. 2025;15(4):301-312. doi:10.4103/jispcd.jispcd_19_25 · PMID 40951721
- Tay JRH, Ng E, Lai CWM, Lim LP, Ong MMA. The efficacy of probiotics in the management of intra-oral halitosis: a systematic review. Clin Oral Investig. 2022;26(7):4687-4700. doi:10.1007/s00784-022-04522-w · PMID 35536439
- Nakano Y, Yoshimura M, Koga T. Correlation between oral malodor and periodontal bacteria. Microbes Infect. 2002;4(6):679-683. doi:10.1016/S1286-4579(02)01586-1
References
Looking for a specialist?
Parodontologia a Frosinone →Diagnosi e trattamento della parodontite nello Studio Denti Più
Need a professional opinion?
Book an appointment at Dr. Bruschi's practice in Frosinone. First visit includes full diagnosis and personalised treatment plan.
Stay Updated
New articles on periodontology, implantology and oral surgery — delivered to your inbox.
Comments
Loading comments...
Leave a comment